
The Bloody Truth
Behind The Barber Pole
Did you know your friendly neighborhood barber once wielded more than just scissors and razors? In medieval Europe, a trip to the barber wasn't just for a fresh trim; it could also involve surgical procedures. That's right! These "barber surgeons" were the go-to for everything from pulling teeth to setting bones, making them surprisingly vital figures in the medical landscape of the time.
And have you ever wondered about the iconic red and white stripes of the barber pole? Now you'll know the fascinating (and slightly gruesome) truth behind it. Those colors aren't just for show – they're a direct throwback to the barber surgeons of old. The red represents blood, a stark reminder of the surgical procedures they performed, while the white symbolizes the bandages used. Who knew a simple barber pole held such a captivating and slightly unsettling history?
Welcome to the 113th edition of ResusNation!

Femoral Lines in a Code?
Stop The Madness
As a seasoned medical professional, I've seen firsthand the critical need for rapid and reliable central access during critical events. Far too often, I witness valuable time wasted and potential complications arising from the pursuit of femoral lines in code situations. The reality is, when every second counts, intra-osseous (IO) lines offer a superior alternative. In my experience, IO placement is not only significantly faster and safer for both the patient and the team, but it also provides immediate access to the central circulation, allowing for the swift administration of essential medications, fluids, and blood products. It's time we moved past outdated practices and embraced the efficiency and reliability of IO access.
Despite being 2024, the underutilization of IO lines continues to be a concern. We have multiple safe and effective insertion sites available – humeral, tibial – providing the ability to establish multi-line access if required. The risks associated with blind femoral line placement during high-pressure situations, including arterial puncture and other complications, simply don't compare to the speed and safety profile of IO insertion. For rapid, reliable central access when it truly matters, the intra-osseous line should be our go-to.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or Linkedin accounts.
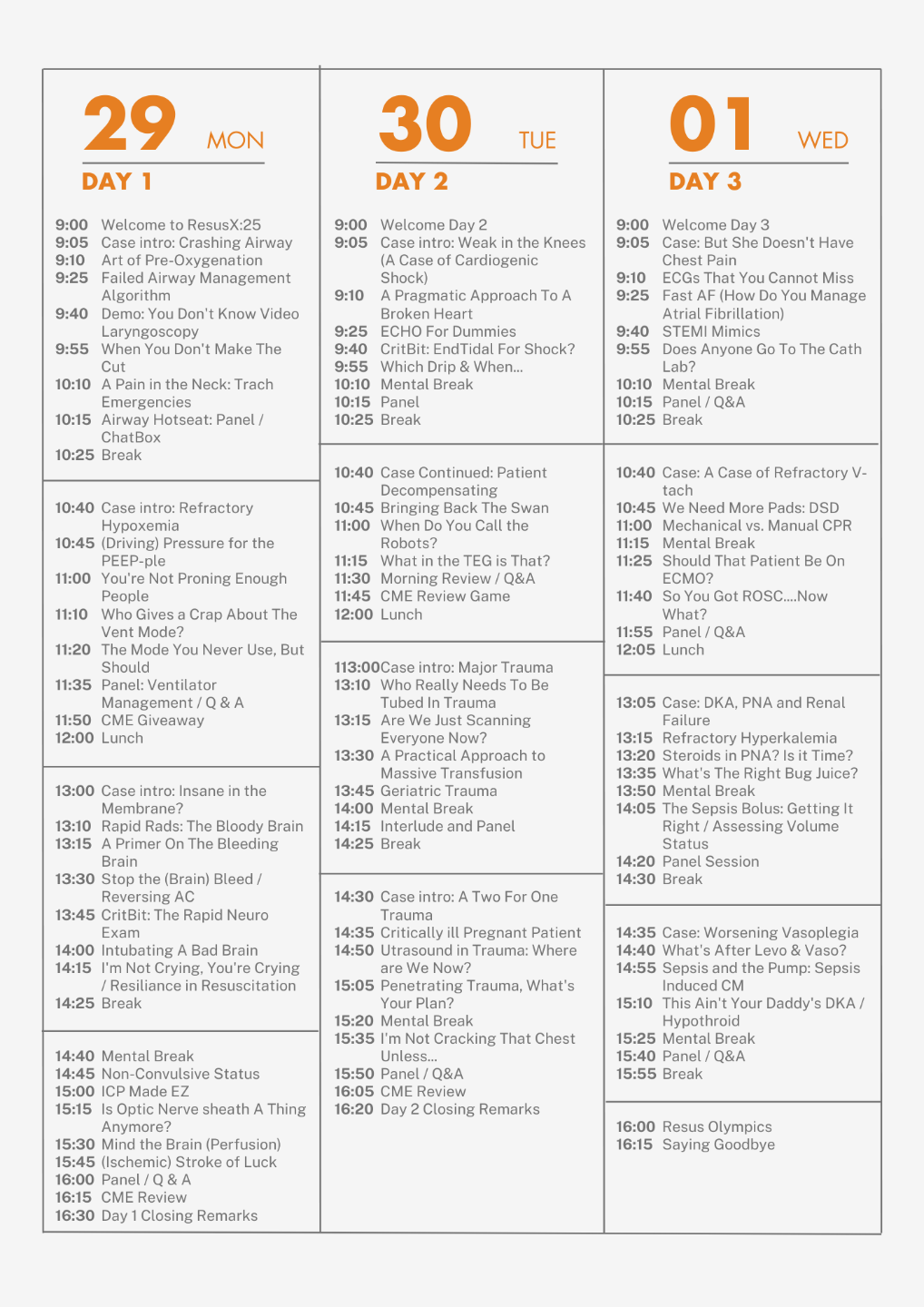
Save 50% off Registration
Last Friday, we opened a limited run of early-bird tickets for Attending and non-Attending physicians. We sold out our allotment of non-Attending tickets in less that 24 hours! These discounted tickets were the cheapest prices we will be offering for this year's conference and we reserved them only for the ResusNation. The good news is that we still have a few of these deeply discounted Attending tickets still available for sale. Again, these are the cheapest tickest that we will be offering for ResusX:2025 and there are only a few left. Here's the link to these tickets.
But don't feel bad if you're a resident, nurse, NP, PA, or paramedic...another limited run of early-bird tickest will go on sale this Wednesday at 9amEST. Set your alarm clocks, because it's first come, first serve for these tickets. Please do not share your code with anyone...this is an exclusive sale for the ResusNation.

Haloperidol for Delirium: Examining the Evidence
Delirium, a state of acute confusion, is a common and distressing complication for patients in the intensive care unit (ICU). This sudden change in mental status can be frightening for patients and their families, and doctors have long sought the best ways to manage it. A recent study published in the New England Journal of Medicine sheds light on the use of haloperidol, a drug frequently used to treat delirium. The research aimed to determine if haloperidol could help patients spend more time alive and out of the hospital. Surprisingly, the study found that haloperidol did not significantly increase the number of days patients lived and were able to leave the hospital compared to a placebo.
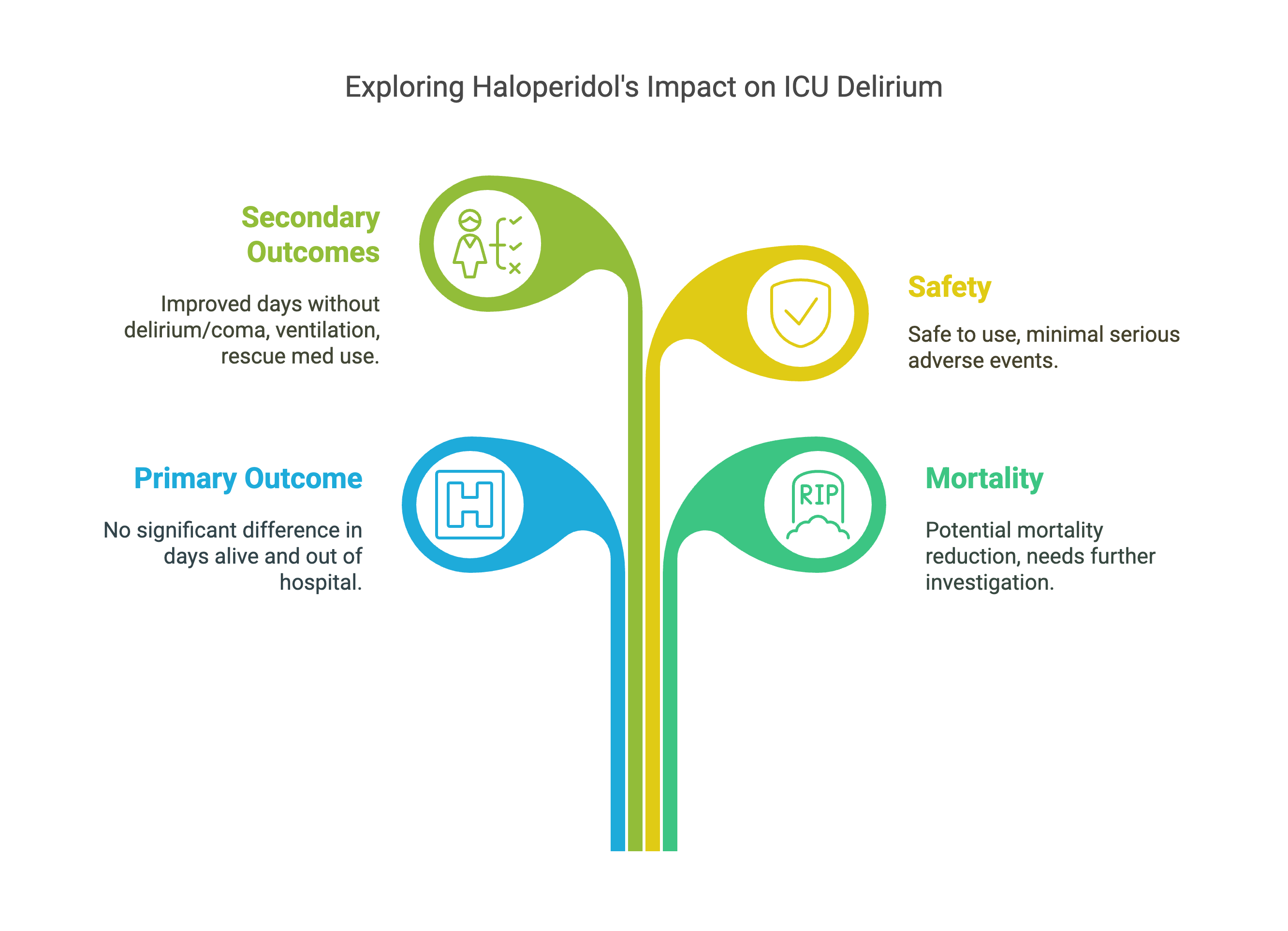
However, the study did reveal that patients treated with haloperidol had a lower risk of death. This is an important finding, although the drug's impact on overall recovery time was not seen. While this research provides valuable insights, it's important to remember that every patient is different. The best treatment approach will always depend on the individual's specific situation. Future research will likely focus on even more tailored strategies to care for patients with delirium in the ICU, aiming to improve both survival and recovery.
Here's my takeaways:
-
Haloperidol's effectiveness is questioned: The study's primary finding suggests that haloperidol may not be effective in increasing the number of days ICU patients with delirium spend alive and out of the hospital.
-
Mortality benefit needs further exploration: While haloperidol didn't improve the primary outcome, the study did indicate a potential benefit in reducing mortality.
-
Need for individualized treatment strategies: The study reinforces the idea that there is no one-size-fits-all solution for managing delirium.
-
Importance of continued research: The authors emphasize the need for ongoing research to identify the most effective interventions for delirium in the ICU.
Want to hear more about it? Listen now as we break down the findings that have the medical community buzzing. Click on the podcast below to dive into this game-changing research.
 |
Want to learn more? Read the full study Haloperidol for the Treatment of Delirium in ICU Patients by Andersen-Ranberg et al. in New England Journal of Medicine.

(Resub Impact Corner is a new column by Dr. Ross Prager (@ross_prager) who will be reviewing research methods, statistics, and all the concepts that have traditionally been taught wrong. Follow Ross on X for more content.)
Research Methods: OR vs. HR vs. RR — What You Need to Know...In Under 3 Minutes!
If you’ve ever wondered whether an odds ratio (OR), risk ratio (RR), or hazard ratio (HR) is the right metric, you're not alone.
Here's the fast, practical breakdown:
-
Risk Ratio (RR) compares probabilities of an event between two groups. Example: The risk of AKI was 10% in the treatment group and 20% in the control group — RR = 0.5.
-
Odds Ratio (OR) compares odds, not probabilities. It’s similar to RR when events are rare, but diverges as event rates increase. It tends to overestimate the association between exposure and outcome.
-
Hazard Ratio (HR) accounts for time to event. It’s used in survival analysis: HR tells you the ratio of event rates at any given point in time.
Rule of thumb:
-
Use RR when you can directly measure risk (RCTs, cohort studies).
-
Use OR for case-control studies or logistic regression models.
-
Use HR for time-to-event data (e.g., mortality at 30 days).
➡️ Want to go deeper? We wrote a full, easy-to-digest guide (with examples of how OR and RR can differ): Read the full post
If you're an All-Access Member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring
- Wright on "The Super Sick SAH"
- Reilly on "CT Head for the Resuscitationist - What is the Approach?"
- Haywood on "NIV Mask Seal"
- Rezaie on "DSI v. RSI"
- Qasim on "Getting to the Heart of the Matter: Breaking Down the Resuscitative Thoracotomy"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW! If you're not, then sign up here.


Are you a member of ResusNation? For less than a cup of coffee, you can get even more content from CriticalCareNow. Digital teaching sessions, podcasts, free video lectures, grand rounds, and so much more can be your today. Come watch on replay all the content that CriticalCareNow does live. Check out the membership options below and decide the right one for you.
Do you want even more resus content anytime you want? For less than a cup of coffee, you can get even more content from @CriticalCareNow. Digital teaching sessions, free video lectures, grand rounds, and so much more can be your today. Come watch on replay all the content that @CriticalCareNow does live.
Check out the membership options below and decide the right one for you.


Get Access To The ResusNation Today!


Responses