

Ur-ine Luck! Medicine
is Much Better Now
From medieval "urine wheels" to the widespread practice of bloodletting, medical history is brimming with fascinating, and often startling, approaches to health and disease. For centuries, physicians relied on visual examinations of bodily fluids, with "uroscopy" becoming a cornerstone of diagnosis. This involved meticulously observing the color, clarity, and even taste of a patient's urine, comparing it to elaborate charts (the "urine wheels") to deduce imbalances in the body's humors – a prevailing theory that governed medical thought for over two millennia. While seemingly crude by today's standards, this practice, along with other now-outdated methods, represented humanity's continuous quest to understand and alleviate suffering.
The evolution of medicine truly accelerated with the advent of germ theory in the 19th century, a groundbreaking discovery that finally revealed the microscopic culprits behind many illnesses. This scientific leap led to revolutionary changes, from the development of antiseptic techniques and vaccinations to the introduction of anesthetics like ether and chloroform, which transformed surgery from an agonizing ordeal into a more manageable procedure. Looking back at these historical medical practices not only highlights the remarkable progress we've made but also reminds us of the dedication and ingenuity of those who, with limited knowledge and tools, laid the foundation for modern healthcare.
Welcome to the 121st edition of ResusNation!
Does Your Hospital Have This LVAD Tool?
When it comes to patients with Left Ventricular Assist Devices (LVADs), getting an accurate blood pressure reading isn't as straightforward as with typical patients. From my extensive experience in critical care, I've seen firsthand how these incredible pumps provide a continuous, linear flow rather than the pulsatile ejection we're used to. This means you won't get a traditional systolic and diastolic reading; instead, you're looking for a mean arterial pressure (MAP). Relying solely on a standard blood pressure cuff will simply not give you the information you need, which is a critical point often overlooked, even by seasoned professionals.
The preferred, and most effective, method involves a Doppler device and a manual sphygmomanometer. You'll place the Doppler in the antecubital fossa to locate and listen for the arterial flow. Once you've found that distinct sound, you then inflate the blood pressure cuff until you lose the Doppler signal. That precise point, where the sound disappears, is your mean arterial pressure. Deflating the cuff and hearing the sound return confirms your reading. For critically ill patients requiring frequent monitoring, an arterial line is undoubtedly the wisest choice to avoid repetitive manual measurements, but for an initial or intermittent assessment, this Doppler-guided technique is essential.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or Linkedin accounts.

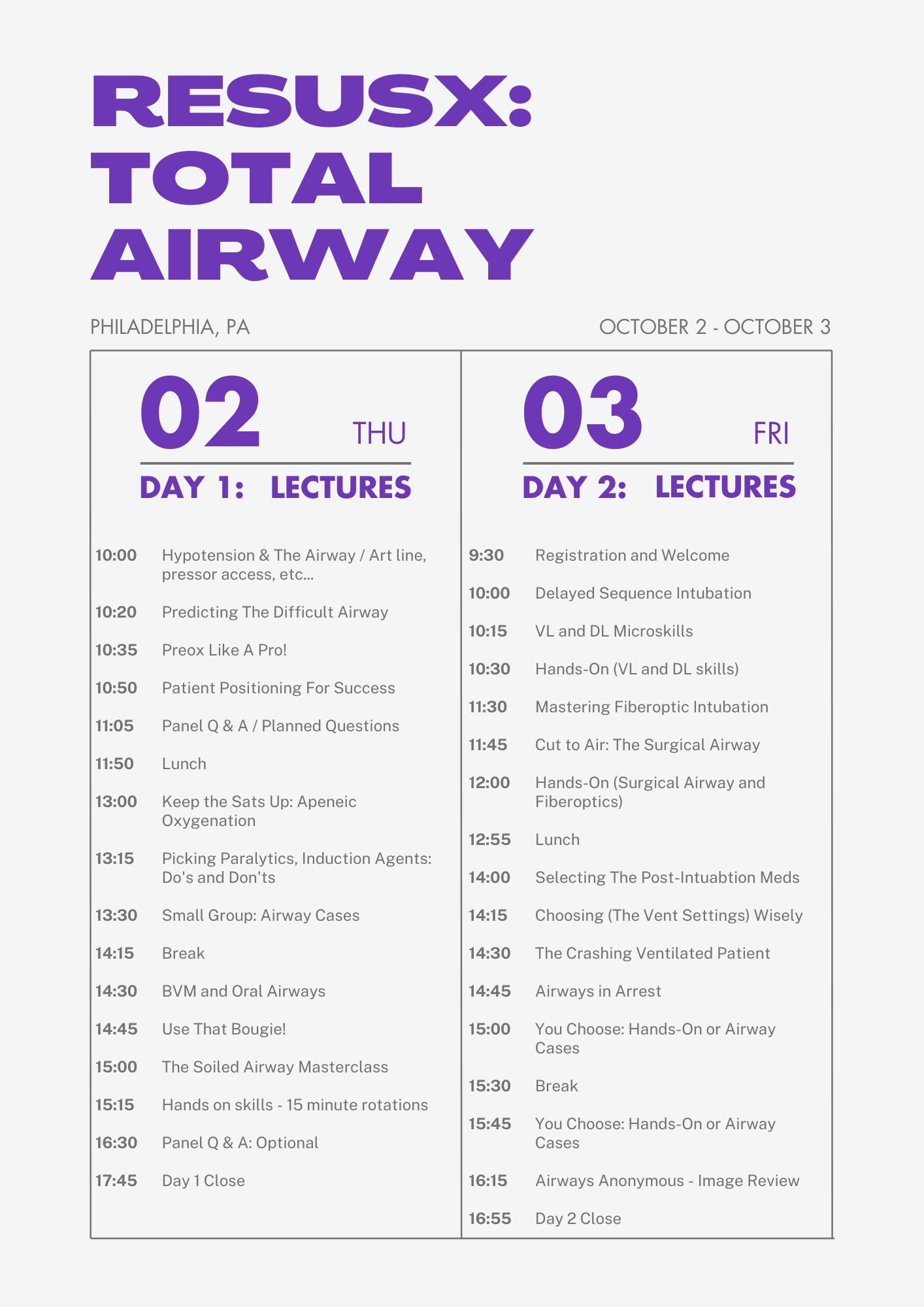
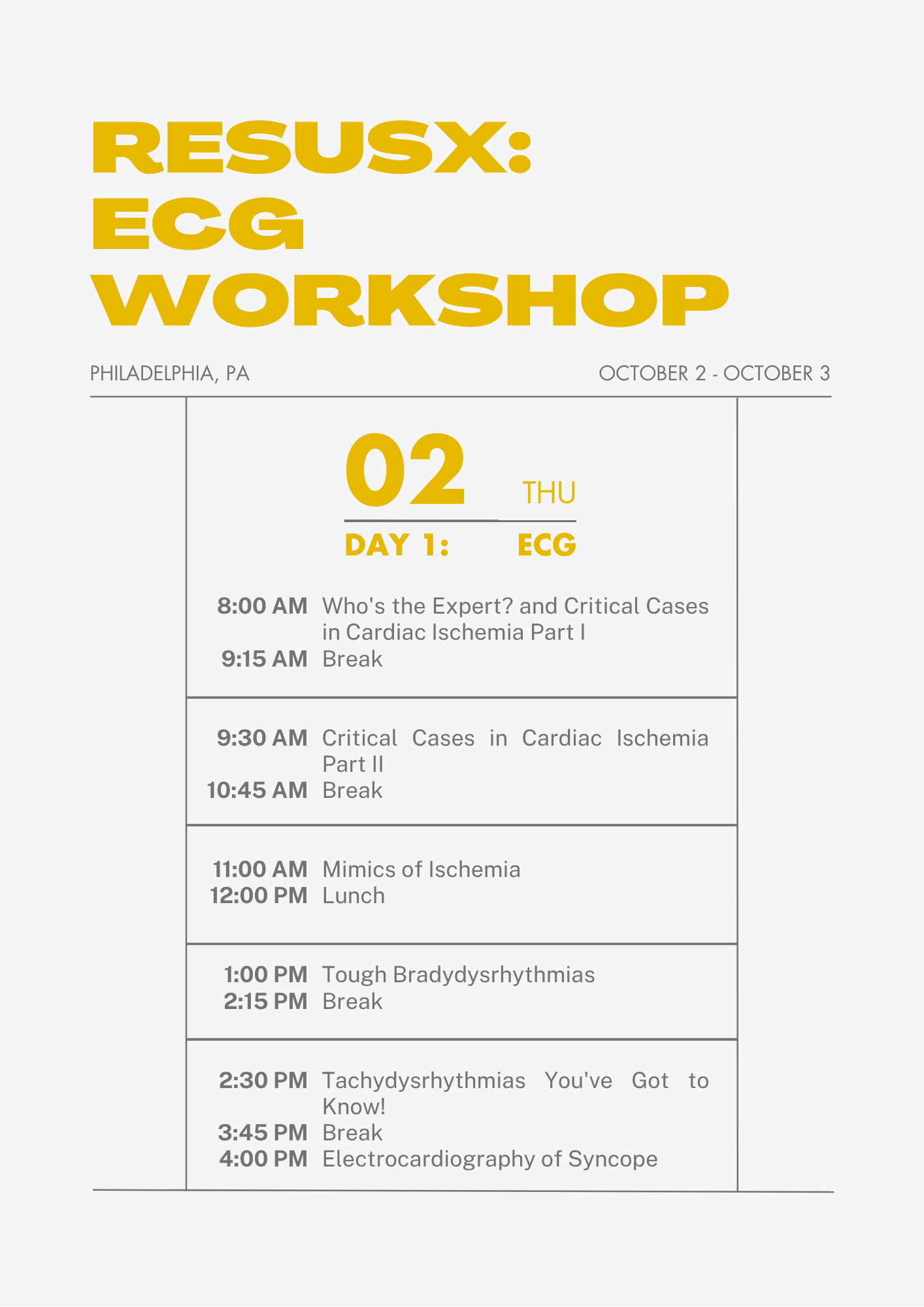
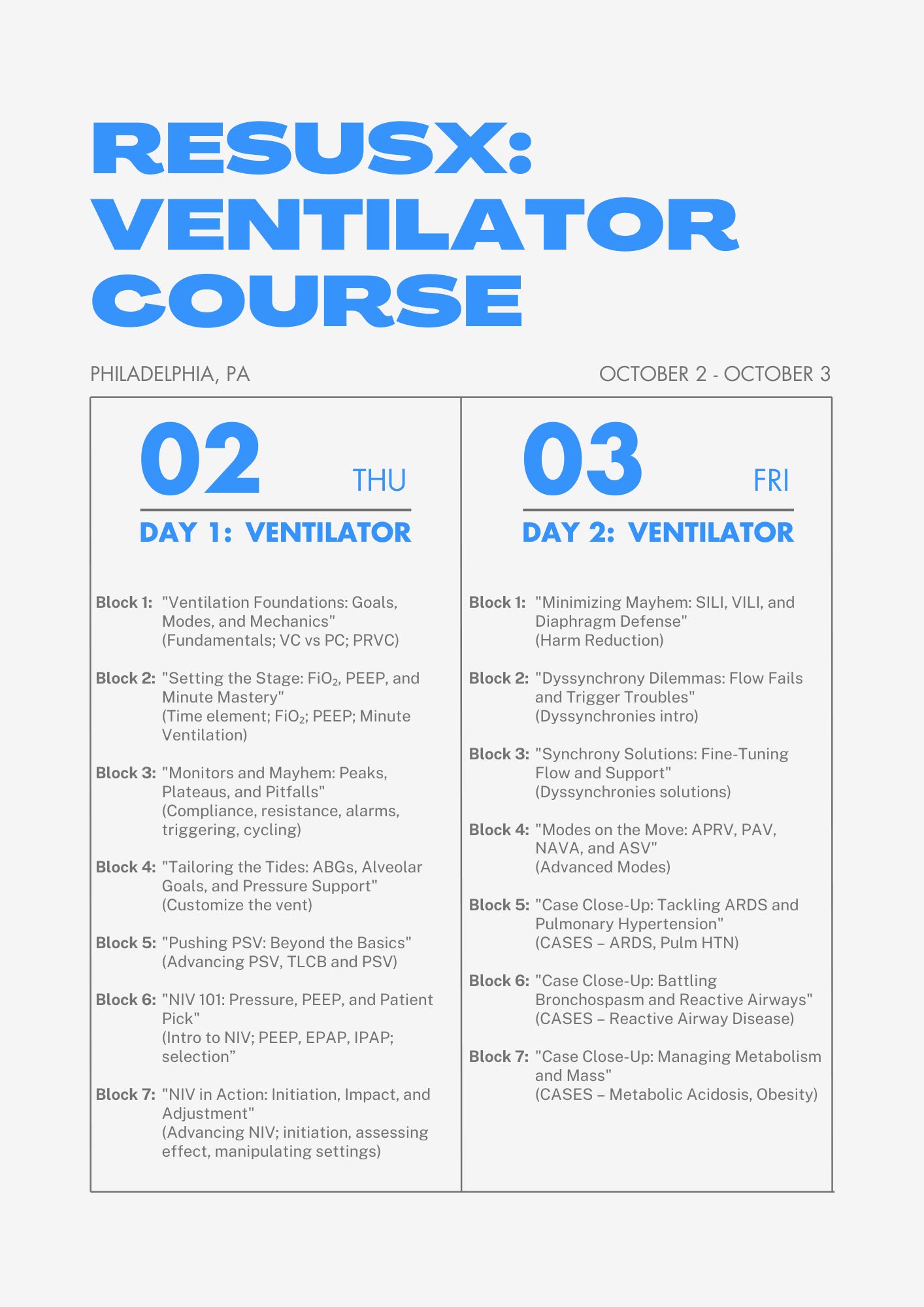
We just launced the ResusX:Workshops series, four incredible hands on workshops that will help you take your ressucitation skills to the next level. Whether you attend these on their own, or part of ResusX, you will level up your skills. Choose from on of the following:
- Total Ariway Workshop
- DysRhythmia Day with Amal Mattu
- Resus:Ready Procedure Workshop
- The Vent Workshop
Full schedules are available below and spots are very limited, so don't wait until the last minute to register!
GET MY TICKET FOR THE WORKSHOP



Why Targeting Lower Oxygen Levels May NOT Be the Answer
For mechanically ventilated patients in the ICU, a common question is how much oxygen is truly beneficial. Historically, more oxygen was often given to prevent low oxygen levels, but recent research has explored whether a more "conservative" approach, providing just enough oxygen, could lead to better outcomes. This is a crucial question because both too little and too much oxygen could potentially cause harm. A large-scale study, the UK-ROX trial, aimed to definitively answer this by comparing conservative oxygen therapy with usual care in thousands of ventilated adults. The main finding? Minimizing oxygen exposure in these patients did not significantly reduce the risk of death at 90 days.
The UK-ROX trial involved 16,500 mechanically ventilated adult patients across 97 ICUs in the UK. Patients were randomly assigned to either receive conservative oxygen therapy, targeting a peripheral oxygen saturation (SpO2) of 90% (with a range of 88%-92%), or usual oxygen therapy, where clinicians decided the oxygen levels. While the conservative group did receive 29% less supplemental oxygen, the study found no meaningful difference in 90-day mortality: 35.4% in the conservative group died compared to 34.9% in the usual care group. There were also no significant differences in how long patients stayed in the ICU or hospital, or how many days they were alive and free from organ support. This means that for the majority of critically ill, ventilated adults, a very strict conservative oxygen target like 90% doesn't seem to offer a survival advantage over current usual practices. While the study was very large and robust, it's important to remember that clinicians could not be blinded to the treatment, and some patients were excluded if the intervention was considered medically necessary or inappropriate. This research provides important clarity, suggesting that current "usual care" oxygen strategies in the ICU are likely appropriate for most ventilated patients, without a need to strictly limit oxygen to very low targets.
Here's my Takeaways:
-
Finding: Minimizing oxygen exposure through conservative oxygen therapy did not significantly reduce all-cause mortality at 90 days in mechanically ventilated critically ill adult patients. The conservative group had a 90-day mortality rate of 35.4% compared to 34.9% in the usual oxygen therapy group, a risk difference of 0.7 percentage points.
-
Practice Impact: The findings do not support the idea that reducing oxygen exposure by targeting a peripheral oxygen saturation (SpO2) of 90% is beneficial for mechanically ventilated adults in the ICU. Current "usual care" oxygen strategies appear to be comparable in terms of patient outcomes.
-
Population: The study included 16,500 mechanically ventilated adult patients receiving supplemental oxygen in 97 ICUs in the UK. The patient population was diverse and representative of a broader ICU population, with a median age of 60 years and 38.2% females in both groups.
-
Limitation: Clinicians and patients could not be blinded to the treatment, and other aspects of care were at the discretion of clinicians. Also, a significant proportion of potential participants were excluded if the intervention was considered indicated or contraindicated by the treating clinician, which might reduce the generalizability of the findings
Want to learn more? Read the full study "Conservative Oxygen Therapy in Mechanically Ventilated Critically Ill Adult Patients" by Daniel S. Martin et al. in JAMA.
Watch the June Videos Now!
If you're an All-Access Member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring
- Wright on "The Super Sick SAH"
- Reilly on "CT Head for the Resuscitationist - What is the Approach?"
- Haywood on "NIV Mask Seal"
- Rezaie on "DSI v. RSI"
- Qasim on "Getting to the Heart of the Matter: Breaking Down the Resuscitative Thoracotomy"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW! If you're not, then sign up here.


Are you a member of ResusNation? For less than a cup of coffee, you can get even more content from CriticalCareNow. Digital teaching sessions, podcasts, free video lectures, grand rounds, and so much more can be your today. Come watch on replay all the content that CriticalCareNow does live. Check out the membership options below and decide the right one for you.
Do you want even more resus content anytime you want? For less than a cup of coffee, you can get even more content from @CriticalCareNow. Digital teaching sessions, free video lectures, grand rounds, and so much more can be your today. Come watch on replay all the content that @CriticalCareNow does live.
Check out the membership options below and decide the right one for you.


Get Access To The ResusNation Today!


Responses