
Welcome to ResusNation #155

Please take this 1 minute survey to help shape the future of the newsletter (click below):
Local Neurons Refuse to Die, Prefer Gaming Instead.
We’ve officially hit the point in the simulation where science fiction writers are starting to look like visionaries or prophets of doom. Researchers have taken a literal handful of human neurons, slapped them onto a multi-electrode array biochip, and essentially told them, "Git gud." By using optogenetic stimulation to provide "sensory" feedback, they’ve trained these lab-grown brain cells to navigate the pixelated corridors of the classic video game DOOM. It turns out that when you give a cluster of cells a dopamine-like reward for not dying and a "punishment" of random noise for hitting a wall, they develop a rudimentary sense of agency faster than a first-year resident learns how to find the hidden snack stash in the ICU. They aren't just firing at random anymore; they are actively processing spatial data to survive a 1993 demon invasion, proving that the urge to play video games is apparently hard-coded into our very biology.
The real kicker isn't just that the "DishBrain" can aim a super shotgun, but what this means for the future of wetware computing and neuro-regeneration. We are looking at a world where your future laptop might literally need a glucose drip and a nap, or where we test new neurologics by seeing if they improve a petri dish's speedrun time. It’s equal parts impressive and existential-dread-inducing to realize that while we’re out here struggling to remember the dosage for amiodarone, a puddle of neurons in a lab is getting better at circle-strafing cyberdemons. It turns out the blood-brain barrier was actually just a suggestion, and the next step in personalized medicine might just be benchmarking your own gray matter against a 30-year-old FPS to see if your synapses are still firing on all cylinders.
Enjoy ResusX, From Anywhere
Can't make it to Philly? No problem.
ResusX:2026 goes live May 18–20 — and you don't need a plane ticket to be in the room. The Virtual Package puts every session on your screen, in real time, the moment it happens.
Same speakers. Same debates. Same procedural demos. You're just watching from a better chair.
Here's what you get:
→ Full livestream of every session — all three days, as it happens. Not highlights. Not a recap blog. The whole thing.
→ On-demand replays so you can pause, rewind, and rewatch the parts that rewire your thinking. At 2am. On your next shift break. Whenever it clicks.
→ Live Q&A — submit questions directly to faculty during sessions.
→ CME and CEU credits — same credits as the in-person attendees. No difference.
→ Expert debates, live procedural demos, real cases, audience polling — the full ResusX experience, streamed to wherever you are.
We're talking resuscitative thoracotomy. Impella placement. Perimortem C-section. Bougie-assisted cric. Proning demos. POCUS for dissection. Three days of the sharpest resuscitation education anywhere — and you won't miss a second of it.
You Got 2 Choices:
→ Conference Pass — $197 (50% off): Livestream access to every session. → All-Access Pass — $397 (50% off): Livestream + on-demand replays so you can revisit everything after the conference ends.
Look — nothing replaces being in that comedy club where the energy is dialed to eleven. We know that. But this is the next closest thing: every minute of content, on your terms, with a replay button.
If you've been telling yourself you'll level up your resuscitation skills "soon" — this is what soon looks like. No flights. No hotel. No asking someone to cover your shifts for three days.

Why Pain Management Comes Before Sedation in the ICU
A mechanically ventilated patient squirming in bed despite maxed-out propofol is likely not a sedation problem, but a pain problem. This is a scenario that plays out more often than it should in the ICU, where the assumption that a patient must have something surgically or traumatically wrong to warrant analgesia can lead to undertreated pain. The reality is that mechanically ventilated patients endure a constant stream of uncomfortable and painful stimuli: endotracheal tubes, blood draws, line placements, immobility, and prolonged bed rest. These patients feel pain regardless of their admitting diagnosis, and failing to address that is both a clinical and an ethical oversight.
The principle of analgesia-first sedation is not just good bedside judgment — it is backed by the SCCM guidelines. Sedatives like propofol carry no analgesic properties whatsoever, and while agents like dexmedetomidine and ketamine offer some analgesic benefit, they are not a substitute for dedicated pain management. When analgesia is prioritized and adequately dosed, the amount of sedation required drops significantly, which translates to better hemodynamic stability and improved patient outcomes. The takeaway is straightforward: before reaching for more sedation in a restless, ventilated patient, always ask what analgesia is on board — and if the answer is little or none, that is where to start.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or LinkedIn accounts.

In this session from ResusX:2025, Dr. Haywood addresses the growing complexity of mechanical ventilation, noting that the alphabet soup of proprietary modes like VAPS and PRVC often triggers imposter syndrome in clinicians. He argues that this focus on advanced, brand-specific technology causes medical professionals to lose sight of the fundamentals that actually dictate improved patient outcomes. By obsessing over closed-loop systems and modern jargon, clinicians frequently overlook basic, evidence-based practices that have been established for over 20 years, leading to preventable errors in critical illness.
To combat this, Dr. Haywood emphasizes three core pillars of ventilator management: 1) maintaining appropriate tidal volumes based on ideal body weight (rather than actual weight), 2) avoiding the hidden dangers of hyperoxia, and 3) utilizing prone positioning for severe ARDS. He highlights a startling statistic—that 40% of patients are still given inappropriately high tidal volumes—and provides a "safe landing area" for PaO2 targets. The ultimate message is a call to return to the basics: measure your patients accurately, start with lower oxygen concentrations, and master the foundational mechanics before worrying about the latest machine-specific features.
Check out this video of Dr. Steve Haywood from ResusX:2025 now!


Axillary vs. Jugular: Time to Rethink Your Default CVC Site?
Central venous access site selection carries real consequences for infection risk and mechanical complications in critically ill patients. The axillary vein (AXV) has been gaining traction as an alternative to the traditional internal jugular vein (IJV) as ultrasound guidance has become standard practice, but head-to-head evidence has historically been fragmented. This systematic review and meta-analysis in Critical Care addresses that gap, drawing on 908 patients across three RCTs and applying trial sequential analysis (TSA) to confirm sufficiency of evidence. The findings are clear: ultrasound-guided infraclavicular AXV cannulation is equivalent to IJV in both efficacy and safety. Overall cannulation success was 95% vs. 98% (RR 0.98; 99% CI 0.95–1.02) — a non-significant difference — and cumulative mechanical complications were identical between sites (RR 1.05; 95% CI 0.69–1.61). First-pass success trended slightly lower with AXV (78% vs. 84%), but TSA and alternative modeling confirmed the difference was negligible.
The clinical implications extend well beyond equivalence. Because the AXV shares the infraclavicular skin exit site with the subclavian vein, it is expected to carry the same reduced rates of catheter-related bloodstream infection (CRBSI) and venous thrombosis that make the subclavian approach guideline-preferred — advantages the IJV cannot offer. Routine AXV use also preserves the right IJV for high-priority large-bore access needs such as dialysis catheters, pulmonary artery catheters, and ECMO cannulae. The authors note that proximal and distal AXV approaches appear equally effective, though safety data for the distal segment warrants further study given lower reported first-pass success rates and the critical importance of adequate catheter length to avoid tip malposition.
My Takeaway Points:
-
Finding - Across 908 critically ill patients in three RCTs confirmed by trial sequential analysis, ultrasound-guided axillary vein cannulation achieved equivalent overall success (95% vs. 98%; RR 0.98) and identical complication rates (RR 1.05) compared to the internal jugular vein, with high-certainty GRADE evidence for efficacy and moderate certainty for safety.
-
Practice Impact - Ultrasound-guided infraclavicular AXV cannulation should be considered a first-line central venous access option in critically ill patients — its infraclavicular skin exit site confers the same lower CRBSI and thrombosis risk as the subclavian approach, while reserving the right IJV for large-bore devices such as dialysis catheters, pulmonary artery catheters, and ECMO cannulae.
-
Population - Mechanically ventilated and non-ventilated critically ill adults across ICU, emergency department, and cardiac surgery settings at multiple European centers, with procedures performed by operators with at least six months of ultrasound-guided cannulation experience.
-
Limitation - The primary analysis did not include catheter-associated infection or thrombosis rates as endpoints due to limited AXV-specific data; the optimal information size for the distal versus proximal AXV secondary analysis was not achieved; and the lack of subclavian vein comparator data limits direct guidance on site hierarchy when all three options are available.
Want to learn more? Read the full review Efficacy and Safety of Ultrasound-Guided Infraclavicular Axillary Vein Cannulation for Centrally Inserted Central Catheter Placement in Critically Ill Patients: Systematic Review with Meta-Analysis and Trial Sequential Analysis by T. Królicki, et al. in Critical Care.
Acute Hyperkalemia: What Actually Works (With and Without ECG Changes)
This week Dr. Jain provides a practical, evidence-based breakdown of managing acute hyperkalemia, emphasizing that the ECG is the central decision-making tool. When significant conduction or rhythm abnormalities are present — such as QRS widening, bradycardia, or ventricular escape rhythms — IV calcium is indicated immediately to stabilize cardiac function, acting within 1–3 minutes without affecting potassium levels. However, calcium is not appropriate for earlier ECG changes like peaked T waves or PR prolongation, and it is not indicated at all when no ECG changes are present. He also challenges two common clinical reflexes: sodium bicarbonate has little potassium-lowering effect unless true metabolic acidosis is present, and loop diuretics are only useful when the kidneys are actually functioning.
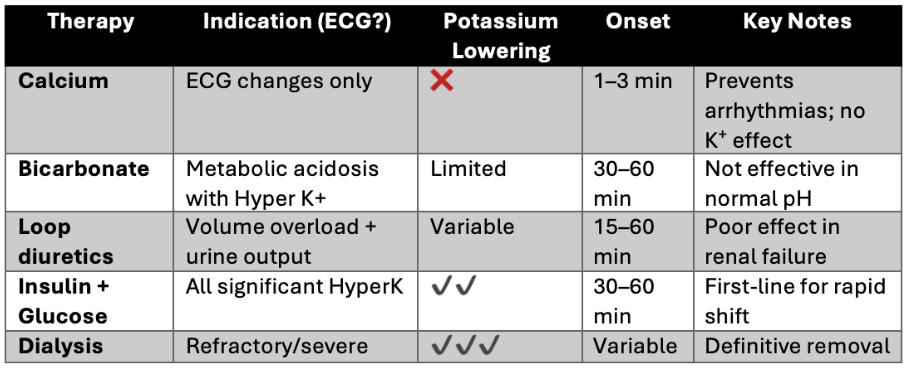
For actually reducing potassium levels, Dr. Jain identifies insulin plus glucose as the fastest and most reliable therapy, capable of dropping potassium by roughly 0.7–1.2 mmol/L within an hour, with nebulized beta-2 agonists offering an additive effect when used alongside it. Dialysis remains the definitive treatment for refractory or severe cases, particularly in patients with significant renal dysfunction. He acknowledges ongoing gaps in the evidence — including a lack of standardized ECG criteria and the recent challenge to calcium's traditional membrane stabilization mechanism — but concludes that a structured, ECG-guided approach can eliminate dangerous delays and unnecessary interventions in what is ultimately a time-critical emergency.
Read the full post here and review this week's Frontline clinical pearls on IG.
----------
Dr. Arihant Jain is an Emergency Medicine physician at All India Institute of Medical Sciences (AIIMS) in New Delhi, and the creator of Life on the Frontline, a blog sharing concise, evidence-based insights from the ED. He currently serves as a Decision Editor for CPC-EM, is among the youngest ATLS faculty in India, and an AHA-certified BLS/ALCS instructor.
Connect with Dr. Jain: @humans.of.em (IG)
Watch the April Videos Now!
If you're an All-Access member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring:
- Rezaie on "How High Can You Go?"
- Repanshek on "Crashing Anaphylaxis"
- Wright on "The Rapid Neuro Exam"
- Quazi on "Resuscitative Hysterotomy"
- Swaminathan on "Fast AF (How Do You Manage Atrial Fibrillation)"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW!


Responses