
Welcome to ResusNation #159
The Beetle Juice That Kills You
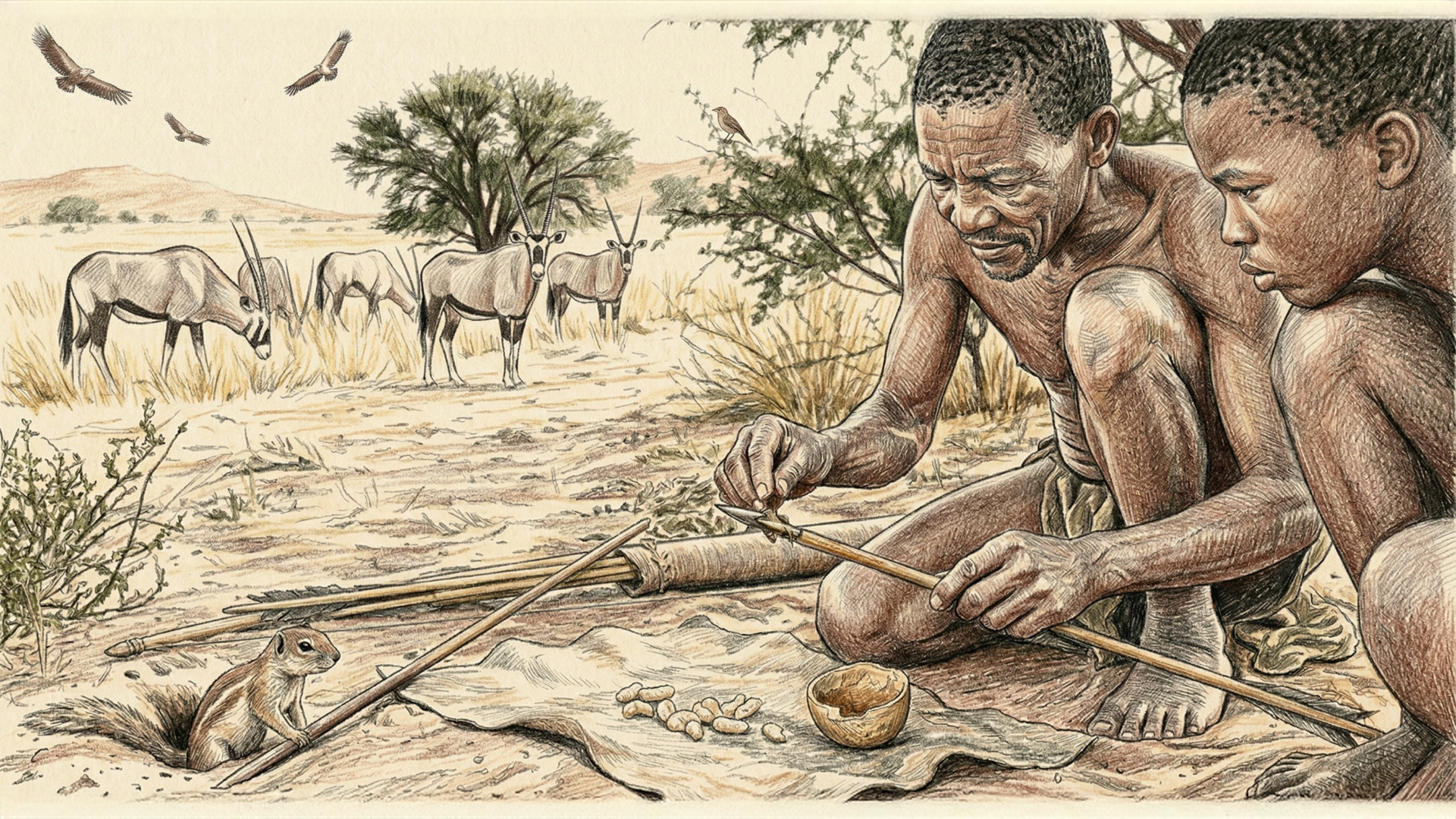
Imagine you’re a Khoisan tracker in the Kalahari, and instead of a pharmacy, your "extra-strength" solution for hunting a wild animal is tucked inside the dirt. Enter the Diamphidia beetle, a creature whose larvae contain a diamphotoxin so powerful it makes rattlesnake venom look like a refreshing electrolyte drink. We aren't just talking about mild irritation here; this is a slow-burn cellular heist. The trackers dig up these grubs and smear the internal contents onto their arrows before a hunt. It’s a low-volume, high-stakes delivery system where the toxin doesn’t just stop the heart; it systematically dismantles the red blood cell membranes and blocks neuromuscular function.
While most toxins are flashy and immediate, Diamphidia is the "slow-is-smooth, smooth-is-deadly" specialist. The toxin works by creating massive, non-selective pores in cell membranes, leading to a catastrophic influx of ions that any targeted animal simply cannot compensate for. It’s the ultimate David vs. Goliath flex: a tiny, underground grub providing the chemical leverage to bring down some of the largest land mammals on Earth. As Dr. Steve Boyes and Werner Herzog capture in their National Geographic documentary, Ghost Elephants, it’s a grimly beautiful reminder that nature doesn't need a lab to develop the perfect weapon—it just needs a really specific beetle and a few thousand years of human ingenuity to figure out exactly how to weaponize its guts.

ResusX:2026 Is Less Than 2 Weeks Away!
Only 23 LIVE tickets left!
ResusX 2026 starts May 18 in Philadelphia — and unlike a hotel ballroom, the Punch Line doesn't keep increasing in size. When the room fills, it fills.
What you'll be in the room for:
→ Live procedural demos. Not clips.
→ Expert debates that actually move the needle.
→ Cases where you're the one making the call.
→ Heavy content. Unforgettable room.
If you've been telling yourself you'll level up your resus skills "soon", there is no later this year. There's just this.
→ Not an attending physician? You're invited too. Get your discount code here.

Is POCUS the Modern Stethoscope?
I'm going to say something that might ruffle some feathers: if you're not utilizing bedside ultrasound in 2026, you are not giving your patients the best care possible. I don't care how many years you've been practicing or how many thousands of patients you've managed — without point-of-care ultrasound (POCUS), you are flying blind. You cannot accurately determine hemodynamic status, you cannot reliably assess fluid needs, you cannot identify reversible causes, and you cannot confirm whether your interventions are actually working. That's not opinion, that's clinical reality.
The good news is you don't need to be an expert sonographer to make this work for your patients. You just need to incorporate the fundamentals into your clinical algorithm. Think of it the way our predecessors thought about the stethoscope — it was once a novel tool that eventually became non-negotiable. We are at that same inflection point with bedside ultrasound right now. If you don't have the skills yet, go to a course, shadow your hospital's sonographers, learn from colleagues who are already doing it. The path forward is clear. In 2026, this is no longer optional — it's standard of care.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or LinkedIn accounts.


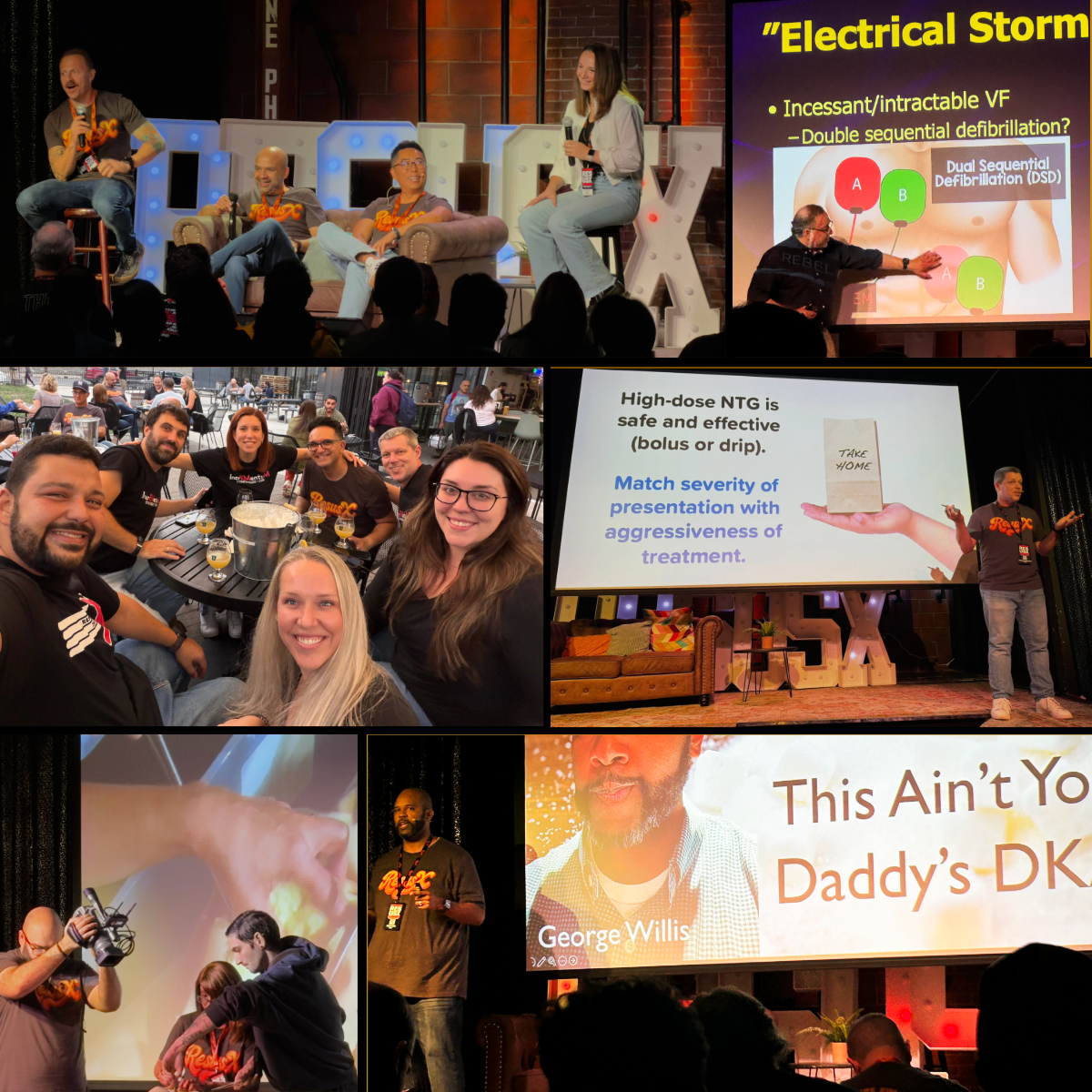
Electrical storm is a rapidly escalating cardiovascular emergency defined by three or more episodes of sustained ventricular tachycardia (VT), ventricular fibrillation (VF), or appropriate ICD shocks within a 24-hour period. As patients with advanced cardiomyopathy and ICDs live longer, the incidence of this condition is rising, creating a vicious cycle driven by a massive surge in sympathetic tone. The pathophysiology is critical: the physical pain of ICD shocks and the physiological stress of the arrhythmia trigger a catecholamine release, which further destabilizes the heart's electrical system, leading to more shocks and more adrenaline. Breaking this adrenergic spiral is the primary goal of modern management.
The shift in treatment strategy focuses on suppressing the sympathetic nervous system rather than relying solely on traditional ACLS protocols. While amiodarone is the preferred antiarrhythmic due to its inherent beta-blocking properties, Dr. Mattu emphasizes the early use of dedicated beta-blockers like propranolol (which crosses the blood-brain barrier to blunt central sympathetic drive) and the use of propofol for sedation due to its unique anti-adrenergic effects. In cases of refractory VF, clinicians are encouraged to de-escalate the use of epinephrine—which can paradoxically worsen the storm—and consider advanced techniques such as dual sequential defibrillation to terminate the lethal rhythm and stabilize the patient.
Check out this video of Dr. Amal Mattu from ResusX:2025 now!


A.I. in Critical Care: A Collaboration?
The modern ICU is drowning in data — continuous monitoring, high-frequency labs, ventilator waveforms, and nursing documentation create an information stream that overwhelms human cognition and fuels both burnout and diagnostic error. Into this environment, artificial intelligence (AI) has arrived with enormous promise, yet despite hundreds of published models and growing regulatory approvals, integration into routine critical care remains limited. This review article argues that the gap in AI use is not primarily a technical failure but a failure of purpose: designing AI to replace clinical judgment rather than augment it is the root cause of adoption stagnation. The authors identify three interlocking barriers — algorithmic integrity failures (distributional shift between academic and community settings, racial bias embedded in training data including pulse oximetry inaccuracy in darker-skinned patients, performance variability even in FDA-cleared systems), a trust deficit driven by "black box" models that erode accountability and clinician autonomy, and systemic hurdles spanning fragmented data infrastructure, misaligned incentives, and absent reimbursement pathways.
The proposed solution is a collaborative framework built around "cognitive unbundling" — strategically delegating computationally intensive work to AI while liberating clinicians for irreducibly human tasks. The authors describe four concrete AI roles: 1) a synthesizer that converts fragmented data streams into coherent patient narratives; 2) a sentinel that delivers explainable, proactive deterioration alerts before conventional thresholds are breached; 3) a simulator that runs personalized "what-if" scenarios before interventions are applied; and 4) a stratifier that identifies clinically meaningful subphenotypes within heterogeneous syndromes like sepsis and ARDS. The framework calls for phased implementation — from institutional natural language processing (NLP) tools to regional federated learning consortia to national surveillance infrastructure — and demands prospective RCT validation before any tool reaches routine clinical use.
My Takeaway Points:
-
Finding - AI adoption in critical care is severely limited despite regulatory approvals, with a multicenter study of seven FDA-cleared diabetic retinopathy systems revealing significant real-world performance variability and potential safety concerns.
-
Practice Impact - The field should abandon the "replacement" design philosophy in favor of a collaborative model — AI handles data synthesis, surveillance, simulation, and phenotyping while clinicians retain authority over judgment, synthesis, and compassionate communication.
-
Population - ICU patients cared for by intensivists in data-intensive environments where cognitive overload, alarm fatigue, and clinician burnout directly threaten patient safety.
-
Limitation - The collaborative framework remains largely conceptual; prospective RCT evidence demonstrating that AI-augmented workflows improve patient-centered outcomes (mortality, ventilator-free days, delirium) over standard care does not yet exist and is explicitly identified as the critical next step.
Want to learn more? Read the full article On the Purpose of Artificial Intelligence in Critical Care Medicine by C. Drudi, et al. in the Journal of Translational Critical Care Medicine.
Inhaled Steriods in Acute Asthma Exacerbation: More Data Than You Think
What's up everyone — the Floating Vent Guy is back! Rather than sticking strictly to vent topics, I'm leaning into pulmonary topics that share common ground with prehospital, ED, hospital, and ICU providers.
I wanted to start my newsletter contribution with a topic near and dear to my heart. There's a lot of dogma surrounding steroid use in asthma — how much, how many days, IV vs. PO, and when to start inhaled steroids. The case for inhaled corticosteroids (ICS) is straightforward: they're delivered directly to where they're needed, generally inexpensive when given via nebulizer, carry minimal risk, and offer real potential benefit.
While systemic steroids remain the cornerstone of acute asthma management, high-dose inhaled corticosteroids given early in the ED are backed by solid evidence — and they're underused.
The Edmonds 2012 Cochrane Review (20 trials, 1,403 patients) showed that ICS in the ED reduced hospital admissions from 32 to 17 per 100 patients treated. The effect was strongest in patients not receiving systemic steroids (OR 0.27), with additional signal when added on top of oral steroids (OR 0.54).
Kearns 2020 updated this with 25 studies and 2,733 patients, finding that high-dose ICS added to systemic steroids reduced admission risk (OR 0.73), with moderate evidence for improved clinical scores and vital signs.
Current GINA guidelines support high-dose ICS within the first hour to reduce hospitalization in patients not receiving systemic steroids (Evidence A). In patients already on systemic steroids, evidence is more variable in adults but more favorable in pediatric patients (Evidence B).
Beyond the data, starting ICS in the ED sends a clear message to the patient: this medication matters. Asthma requires ongoing anti-inflammatory treatment — not just a rescue inhaler when things go wrong. Given the safety profile, even a modest chance of benefit justifies use. The risk approaches zero. The potential upside is real. There is no good reason to defer it.
The Real Gap in Practice: We Keep Treating ICS Like an Outpatient Problem
Here's my soapbox moment.
Inhaled corticosteroids are the foundation of asthma management. They're part of the reason shorter oral steroid courses work. Yet in the ED and on the inpatient side, ICS are consistently treated as someone else's responsibility — a follow-up issue, a primary care problem, an outpatient prescription. The patient gets a 5-day prednisone course and nothing else. And then they come back.
Yes, inhalers can be confusing. Yes, they can be expensive. But the benefit is real and the risk is negligible — deferring ICS at discharge or admission is hard to justify when the evidence is staring us in the face.
Here's what I've observed: patients who use nebulizers understand that their treatment matters. They engage with it. That moment — when they're already holding a nebulizer mask — is the perfect opportunity for education. They're familiar with the neb. Now is the time to reinforce that taking a daily inhaled steroid is just as important as reaching for oral steroids when they're feeling bad. One puts out the fire. The other keeps it from starting.
So the next time you're discharging someone from the ED or admitting a patient to the hospital on oral steroids for an asthma exacerbation — add an inhaled steroid. Right then. Don't defer it.
Review this week's pearls on IG.
----------
Dr. Nicholas Ghionni (Floating Vent Guy) is a Pulmonary and Critical Care attending physician, nationally recognized vent educator, and host of The Peak Inspiration Podcast. He is passionate about translating complex ventilator mechanics and physiology into practical bedside education through engaging content, and a year-long ventilation preceptorship based out of the NIH.
Connect with Dr. Ghionni: @pulmtoilet IG / YT / Spotify / Apple
Watch the May Videos Now!
If you're an All-Access member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring:
- Willis on "The Crashing Aortic Dissection Patient"
- Rempell on "Is Optic Nerve Sheath Even A Thing?"
- Byrne on "Intubating The Bad Brain"
- Zanotti on "Conflict Management in the ICU/Slides"
- Salzman on "Intralipid and HDI"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW!


Responses