
Welcome to ResusNation #156
Thank you to everyone who completed the survey. Exciting changes coming soon!
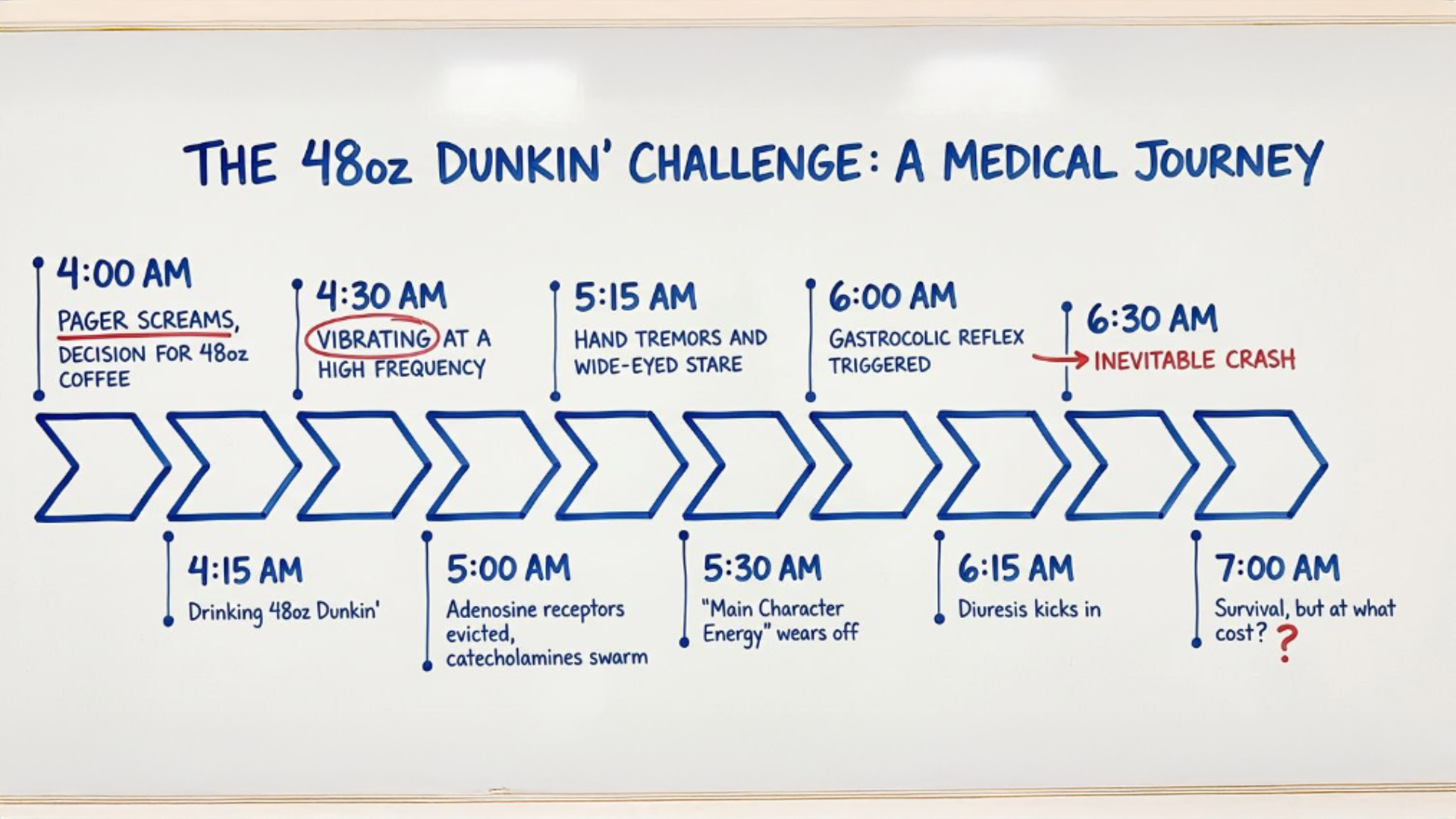
The 48oz Dunkin' Challenge:
A Medical Journey
Dunkin' is now testing 48-ounce "buckets" — complete with a handle and oversized straw — for iced coffee, lattes, and Refreshers at select locations in New Hampshire and Massachusetts. Born from viral social media trends and already selling out at pilot stores, this vessel transforms casual caffeine consumption into a pharmacological event. Adenosine receptor blockade at this dose triggers a compensatory catecholamine surge, driving tachycardia, tremors, and pupillary dilation significant enough to compromise fine motor tasks like central line placement. The caffeine-induced anxiety, osmotic diuresis, and gastrocolic reflex activation that follows ensures that every organ system south of the diaphragm registers its formal objection. What begins as a neurochemical bid for superhuman alertness at 4:00 AM rapidly devolves into a full-body reckoning with stimulant pharmacokinetics.
The aftermath is predictable and merciless. Once the sympathomimetic high fades, the crash doesn't return you to baseline so much as it deposits you in a subterranean pit of irritability, fatigue, and existential regret. Heart rate variability remains deranged, the ECG takes on an alpine quality, and the GI tract harbors a grudge that can persist for three to five business days. The half-life of caffeine will do its job eventually, but not before reminding you that the line between "therapeutic" and "toxicological" is thinner than the foam on your third consecutive latte — or in this case, your first and only bucket.
Enjoy ResusX, From Anywhere
Can't make it to Philly? No problem.
ResusX:2026 goes live May 18–20 — and you don't need a plane ticket to be in the room. The Virtual Package puts every session on your screen, in real time, the moment it happens.
Same speakers. Same debates. Same procedural demos. You're just watching from a better chair.
Here's what you get:
→ Full livestream of every session — all three days, as it happens. Not highlights. Not a recap blog. The whole thing.
→ On-demand replays so you can pause, rewind, and rewatch the parts that rewire your thinking. At 2am. On your next shift break. Whenever it clicks.
→ Live Q&A — submit questions directly to faculty during sessions.
→ CME and CEU credits — same credits as the in-person attendees. No difference.
→ Expert debates, live procedural demos, real cases, audience polling — the full ResusX experience, streamed to wherever you are.
We're talking resuscitative thoracotomy. Impella placement. Perimortem C-section. Bougie-assisted cric. Proning demos. POCUS for dissection. Three days of the sharpest resuscitation education anywhere — and you won't miss a second of it.
You Got 2 Choices:
→ Conference Pass — $247 (40% off): Livestream access to every session. → All-Access Pass — $479 (40% off): Livestream + on-demand replays so you can revisit everything after the conference ends.
Look — nothing replaces being in that comedy club where the energy is dialed to eleven. We know that. But this is the next closest thing: every minute of content, on your terms, with a replay button.
If you've been telling yourself you'll level up your resuscitation skills "soon" — this is what soon looks like. No flights. No hotel. No asking someone to cover your shifts for three days.

3 Tips Every Resuscitationist Needs in Cardiac Arrest
Ultrasound is one of the most powerful tools we have during cardiac arrest — it helps identify reversible causes quickly and can genuinely change outcomes. But here's the thing nobody talks about enough: it can also cause harm. Every second the ultrasound probe is on the chest is a second without compressions, and research shows rhythm checks with ultrasound can stretch to 21 seconds. That's not a minor inefficiency — that's time the patient isn't getting the CPR they need.
After years of running codes and using point-of-care ultrasound, I've landed on three non-negotiables: 1) have the charge nurse count backwards from 10 so everyone in the room knows where you are in the rhythm check, 2) put your most experienced sonographer on the probe — this is not a teaching moment, it's about speed-and-accuracy — and 3) clip first, interpret later. Don't let something interesting on the screen pull your attention while the clock runs. Get the images, get off the chest, and review during the next compression cycle. Good old-fashioned CPR still saves lives. Ultrasound should help that, not compete with it.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or LinkedIn accounts.

Vasoplegia is a refractory state of distributive shock characterized by a "double hit" of profound vasodilation and impaired vasoconstriction, often leaving clinicians frustrated as standard fluid boluses and multiple vasopressors fail to improve blood pressure. A critical diagnostic pitfall involves the hyperdynamic left ventricle seen on ultrasound; while it appears underfilled, it is often reacting to a massive loss of afterload or "POCUS fakes" like right ventricular failure or mitral regurgitation. The core physiological issue is the shift of volume from stressed to unstressed states, where fluid enters a non-pressurized "sink" in the venous system, rendering traditional volume resuscitation ineffective and potentially harmful.
To manage this complex state, Dr. Crager argues that clinicians should move beyond simple fluid administration and adopt a six-step protocol. This strategy includes diversifying vasopressor mechanisms (adding vasopressin or angiotensin II), administering steroids, and correcting metabolic derangements such as hypocalcemia, acidemia, and inappropriate bradycardia. When these interventions fail, rescue therapies like Methylene Blue or Cyanokit serve as a final line of defense by bypassing traditional adrenergic pathways to directly inhibit the vasodilatory cascade, providing a necessary "pressurized" fix to the circulatory system.
Check out this video of Dr. Sara Crager from ResusX:ReUnion now!

 Is The IVC Actually Guiding Your Fluid Decisions, or Just Misleading Them?
Is The IVC Actually Guiding Your Fluid Decisions, or Just Misleading Them?
Fluid responsiveness assessment is central to critical care resuscitation, yet over- or under-resuscitating carries real mortality consequences. IVC ultrasonography became widely adopted for its speed, low cost, and intuitive appeal, but this 2026 narrative review challenges its use as a standalone tool. After synthesizing evidence from PubMed, Embase, Web of Science, and Scopus spanning January 2010 to October 2025, the authors find significant heterogeneity across meta-analyses — with AUCs ranging from 0.43 to 0.92 depending on the study. They also note that IVC ultrasonography fails under conditions common in modern ICUs, such as lung-protective ventilation with low tidal volumes, while operator variability runs 15%–25%. The conclusion: IVC ultrasonography should not guide fluid therapy in isolation.
The review proposes a five-step, physiology-first framework that repositions IVC findings as one contextual signal among many. Clinicians should clear confounders, perform baseline multimodal POCUS including lung ultrasound and focused echo, then use functional maneuvers like passive leg raising with real-time VTI/CO monitoring. VExUS scoring should then be used to grade venous congestion and signal when to stop fluid administration. Only if responsiveness and tolerance both support it should a small, reversible bolus of 250–500 mL be given with immediate re-evaluation. IVC indices should be treated as trend signals rather than fixed thresholds, with action guided by concordance across multiple modalities.
My Takeaway Points:
-
Finding - IVC ultrasonography demonstrates highly variable diagnostic accuracy across real-world settings, with AUCs ranging from 0.43 to 0.92 depending on patient population and conditions — making standalone use clinically unreliable.
-
Practice Impact - IVC measurement should be retired as a primary decision-making tool for fluid therapy and replaced by a multimodal approach: passive leg raising with LVOT VTI/CO as first-line, paired with lung ultrasound for tolerance and VExUS for congestion grading.
-
Population - Critically ill adult patients in ICU and emergency department settings, particularly those on lung-protective ventilation (tidal volume 6–8 mL/kg), with spontaneous breathing efforts, right heart dysfunction, elevated intra-abdominal pressure, or arrhythmias — representing the majority of real-world ICU patients.
-
Limitation - This is a narrative review, not a meta-analysis or RCT, and no patient-outcome–level evidence currently demonstrates that IVC-guided fluid management improves mortality or organ function compared to standard care — a critical evidence gap the authors explicitly flag.
Want to learn more? Read the full review Ultrasound of the Inferior Vena Cava for Fluid Therapy Decisions: Strengths, Limitations, and an Integrated Approach by X. Guo, et al. in Journal of International Medical Research.
Auto-PEEP: The Hypotension You Created
Five minutes after intubation, the blood pressure drops. The patient becomes tachycardic. The ventilator looks “fine.” But before you reach for more pressors, consider this:
You may have just created auto-PEEP.
Auto-PEEP is dynamic hyperinflation. The patient does not fully exhale before the next breath begins. Pressure stacks, venous return falls, and hemodynamics worsen.
Here is how to approach it systematically using the same framework I teach for vent alarms.
1. CONFIRM
Start with the ventilator screen:
-
Is the displayed total PEEP higher than the set PEEP?
-
Is the expiratory flow waveform returning to baseline before the next breath?
If total PEEP exceeds set PEEP and flow never reaches baseline, assume air trapping.
2. ASSESS
Look at the patient. Are there signs of significant auto-peep, including:
-
Tachycardia
-
Hypotension
-
Agitation
-
Difficulty triggering breaths
-
Worsening SpO₂ or rising EtCO₂
3. INVESTIGATE
-
Ask why exhalation is incomplete.
-
Respiratory rate too high
-
Inspiratory time too long
-
Obstruction - e.g. COPD, asthma, mucus plug
-
Ventilator asynchrony and breath stacking
4. INTERVENE
Match the intervention to the cause:
-
Suction early
-
Treat bronchospasm aggressively. Metered-dose inhalers through the ventilator are less effective. Increase dose and frequency.
-
Increase the I:E ratio by:
-
Decreasing respiratory rate
-
Decreasing inspiratory time
-
If this is not working, consider deeper sedation or paralysis to stop breath stacking
-
If the patient is extremely unwell, consider disconnecting from the vent, and manually compress their chest (squeeze their chest hard), to expel trapped air.
5. REASSESS
Recheck total PEEP versus set PEEP, watch the expiratory waveform, and look for hemodynamic improvement.
THE BOTTOM LINE
Auto-PEEP is not rare, and it is often iatrogenic. When hypotension follows intubation, look at total PEEP and the expiratory flow waveform before immediately escalating pressors.
Review this week's Vent pearls on IG.
----------
Dr. Shawn Segeren is a Canada-based Emergency Medicine physician and founder of Dynamic Simulation, a CME-accredited clinical simulation program delivering interprofessional, critical care simulations in emergency departments across Ontario.
Connect with Dr. Segeren: @drsegeren (IG) or @dynamicsimeducation (IG)
Watch the April Videos Now!
If you're an All-Access member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring:
- Rezaie on "How High Can You Go?"
- Repanshek on "Crashing Anaphylaxis"
- Wright on "The Rapid Neuro Exam"
- Quazi on "Resuscitative Hysterotomy"
- Swaminathan on "Fast AF (How Do You Manage Atrial Fibrillation)"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW!


Responses