
Welcome to ResusNation #151

Forget Aspirin, We’re Drinking Awamori Now (Kidding... Mostly)
If you thought your nightly wind-down was just about forgetting the sheer volume of pending notes in your EMR inbox, science has some surprisingly classy news for your cardiovascular system. Honkaku Shochu and Awamori—Japan’s elite single-distilled spirits—aren't just sitting there looking pretty; they’re out here acting like a low-key spa day for your blood vessels. Unlike your standard bottom-shelf vodka that offers nothing but a headache and regret, these spirits have been shown to significantly boost the body’s production of urokinase-like plasminogen activator (uPA), the enzyme responsible for kicking fibrinolysis into high gear. It’s essentially the biological equivalent of hiring a professional cleaning crew to scrub down your intravascular walls while you’re busy debating whether to order another round of gyoza.
Even the mere aroma of these spirits seems to have a measurable effect on fibrinolytic activity, which is a win for anyone who enjoys the "nose" of a good drink as much as the burn. Although Shochu and Awamori are not the only types of alcohol that increase clot-busting enzymes, they were found to have the greatest amount of enzyme activation when compared to whiskey, beer, and wine. However, some studies suggest that long-term, heavy alcohol consumption can lead to reduced fibrinolytic potential. While we aren't exactly writing prescriptions for "Okinawan Moonshine QHS" just yet, it’s nice to know that while the healthcare system tries to give us all a stroke, our choice of beverage might actually be trying to prevent one.
The Medical Conference That Hides Out At A Comedy Club
ResusX 2026 is May 18–20 in Philadelphia — and it's not at a hotel ballroom.
It's at the Punch Line Comedy Club. Intimate seating. A stage close enough to catch every move of a live procedural demo. A room literally engineered to hold attention — which means the energy at 2pm hits the same as 9am.
What's happening:
- Tight, high-momentum sessions built around actual learning
- Live demos (not clips, not diagrams)
- Real expert debates that sharpen how you think
- Interactive formats where you're making the calls
Heavy topics. Unforgettable delivery.
If you've been meaning to level up your resuscitation skills, this is the one worth clearing your calendar for.
Lock in your spot at ResusX 2026
→ Not an attending physician? You're still invited. Fill out this form to unlock a discount code built for non-attending clinicians.
From Controversy to Consensus: The Case for Steroids in Septic Shock
Steroids, specifically hydrocortisone, are used in septic shock for patients who remain in refractory vasopressor-dependent shock. There are three core reasons for their use. First, septic shock causes a relative adrenal insufficiency, where the adrenal glands cannot produce enough cortisol to meet the body's demands, and hydrocortisone replaces that deficit. Second, steroids improve vascular tone by sensitizing adrenergic receptors on blood vessel walls, which enhances venoconstriction and arterial tone, ultimately allowing patients to achieve adequate blood pressure with lower vasopressor doses. Third, and most importantly, steroids help modulate the cytokine storm that occurs in sepsis, where the pro-inflammatory cascade overshoots its protective purpose and begins causing end-organ damage and increased mortality. The overall goal of steroid therapy is not to eliminate the inflammatory response entirely, but to temper it enough to prevent it from causing further harm to the patient.
The use of steroids in septic shock has been debated in the medical literature for decades, with studies going back and forth on whether they improve mortality. Landmark 2018 APROCCHSS and ADRENAL trials have shifted the consensus toward supporting their use in vasopressor-refractory septic shock, showing both mortality benefit and faster shock reversal. The regimen typically includes hydrocortisone, with some debate around the addition of fludrocortisone, as APROCCHSS included it and demonstrated benefit while ADRENAL did not use it. A 2024 meta-analysis of 45 RCTs found that corticosteroids probably reduce mortality and increase shock reversal, but they also may increase the risk of hyperglycemia, hypernatremia, and neuromuscular weakness.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or Linkedin accounts.

In this high-yield clinical breakdown from ResusX:2025, Dr. Willis challenges the standard management of DKA when it intersects with critical illness, respiratory distress, and AKI. Moving beyond the SQuID protocol for mild-moderate cases, he identifies the risk of intubating severely acidotic patients, where a failure to match minute ventilation can lead to rapid cardiovascular collapse. Instead, he advocates for a hierarchy of oxygenation, prioritizing high-flow nasal cannula and non-invasive positive pressure ventilation (NIPPV) to support respiratory compensation.
When it comes to resuscitation, the "Willis Rule" and ultrasound-guided fluid management take center stage to prevent the pitfalls of refractory hyperkalemia and fluid overload, respectively, especially in renal failure. Dr. Willis emphasizes the shift toward balanced crystalloid solutions and the proactive use of the "two-bag system"—adding dextrose to maintain insulin infusions rather than down-titrating the insulin itself. By treating the underlying etiology, such as sepsis secondary to pneumonia, and carefully navigating the potassium-insulin-glucose relationship, clinicians can stabilize even the most metabolically deranged patients.
Check out this video of Dr. George Willis from ResusX:2025 now!


Admit the Person, Not Just the Problem: Moving Away from Reflexive ICU Admission
Every day, clinicians face one of medicine's hardest questions: which patients actually benefit from ICU admission? A 2026 narrative review by Haydon and Brown in the Journal of Critical Care argues that the two ethical frameworks most commonly used to guide ICU admission decisions — the "rule of rescue" and clinical futility — are both inadequate for real-world triage. Reflexively admitting the sickest patient ignores that ICU survival often means loss of functional independence, while futility as a threshold is too binary to apply consistently: fewer than half of ICU clinicians agreed on a less-than-1% survival threshold as grounds for declining admission. Compounding this, surrogates correctly predict patient preferences only 68% of the time, and physicians accurately predict patients' willingness to accept nursing home care just 18% of the time — exposing a profound gap between assumed and actual patient values.
The authors propose proportionality as a more ethically defensible alternative, requiring clinicians to weigh treatment burdens against the likelihood of outcomes the patient would genuinely value, while accounting for clinical context and resource constraints. They pair this with Moral Case Deliberation (MCD), a structured ethics tool that brings the care team together for shared reasoning and collaborative decision-making — shown to reduce interprofessional conflict and build ethical reasoning capacity. The core message: ICU admission should be driven not by what medicine can do, but by a rigorous, goal-informed analysis of what it ought to do.
My Takeaway Points:
- Finding - Surrogates predict patient treatment preferences accurately only 68% of the time, and physicians correctly estimate patients' willingness to accept institutional care just 18% of the time — exposing a critical gap in how ICU goals-of-care decisions are currently made.
- Practice Impact - Replace futility-based and rescue-driven triage reasoning with a proportionality framework that explicitly integrates patient goals, physiological reserve, severity of illness, and available resources — and support this with structured MCD to build team decision-making capacity.
- Population - Particularly relevant for frail, elderly, or multimorbid patients (e.g., 83-year-old with sepsis and multiple comorbidities) in any resource-constrained ICU setting where admission thresholds require more than the absence of futility.
- Limitation - This is a narrative review, not a clinical trial — it synthesizes ethical frameworks and qualitative evidence rather than providing outcome data, and proportionality demands a level of ethical literacy and communication skill that many clinicians have not been formally trained to deliver.
Want to learn more? Read the full article Proportionality and the Process of Decision Making Around ICU Admission: A Narrative Review of the Ethical Complexities of Navigating From "Can" to "Ought" by T. Haydon et al. in Journal of Critical Care.
The Heart Failure Syndrome
This week Dr. Jain challenges the common emergency department habit of reflexively treating every heart failure presentation with furosemide (Lasix). The central argument is that heart failure is a syndrome with distinct hemodynamic phenotypes — not a single disease with a one-size-fits-all protocol. He outlines three clinically relevant phenotypes: the cardiogenic phenotype (true pump failure with low output and hypoperfusion, where aggressive diuresis can cause harm), the vasogenic phenotype (afterload mismatch, subdivided into SCAPE — a sudden, hypertensive flash pulmonary edema driven by a sympathetic surge — and FOSPE, a more gradual volume and afterload problem), and the congestive/volume-overload phenotype, where loop diuretics genuinely are the right treatment.
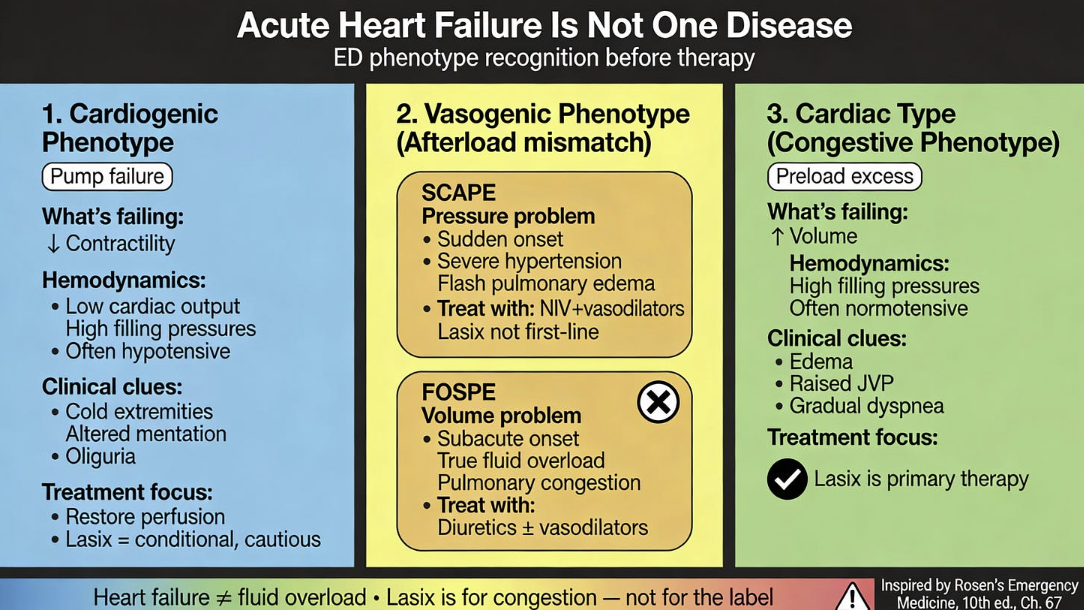
Dr. Jain’s main takeaway is to be aware of the “Lasix fallacy" — the tendency to equate a heart failure diagnosis with fluid overload and automatically reach for diuretics. Citing guidelines from the European Society of Cardiology and recent literature, he emphasizes that loop diuretics are indicated for heart failure with clinical congestion, not universally. The practical implication for clinicians is to shift the question from "does this patient have heart failure?" to "which failure is dominant right now — pump, pressure, or volume?" — and to use POCUS as an adjunct to differentiate phenotypes before committing to a treatment approach.
Read the full post here and review this week's Frontline clinical pearls on IG.
----------
Dr. Arihant Jain is an Emergency Medicine physician at All India Institute of Medical Sciences (AIIMS) in New Delhi, and the creator of Life on the Frontline, a blog sharing concise, evidence-based insights from the ED. He currently serves as a Decision Editor for CPC-EM, is among the youngest ATLS faculty in India, and an AHA-certified BLS/ALCS instructor.
Connect with Dr. Jain: @humans.of.em (IG)
Watch the March Videos Now!
If you're an All-Access member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring:
- Hedayati on "Resuscitate Before You Intubate"
- Zanotti on "The Fearless ICU"
- Gutierez on "Which Drip & When...(Part II)"
- Willis on "Refractory Hyperkalemia"
- Winters on "Serious Slip-Ups In Sepsis"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW!


Responses