
Welcome to ResusNation #158
Ctrl+C, Ctrl+V: The 20-Year Mouse Glitch
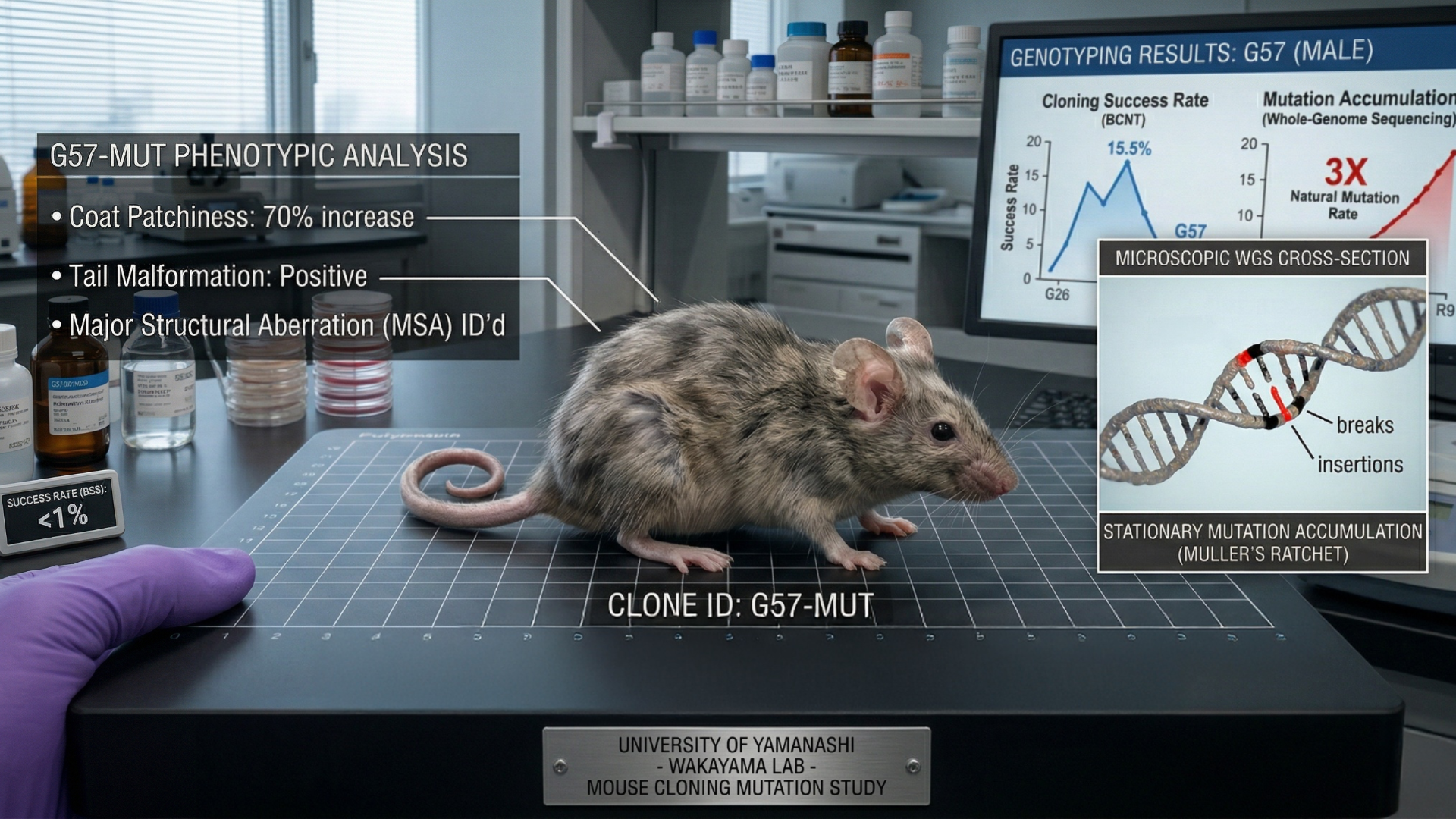
Imagine you’ve been copying the same homework assignment since 2005, but every time you hit print, the ink gets blurrier and blurrier. That is essentially what Japanese researchers did over a two-decade-long bender of somatic cell nuclear transfer. They started with one female mouse and just kept hitting the “clone” button, birthing over 1,200 rodents across 58 generations. For the first 25 rounds, things were actually looking promising—the mice were healthy, the success rates were climbing, and everyone thought we’d finally cracked the code for an infinite army of identical lab rats. It was the ultimate "nothing can go wrong" moment in science, right up until the genome decided it was time to self-destruct.
By the time the team reached the 58th generation, the vibe shifted from "scientific breakthrough" to "biological horror movie." The clones hit a genetic dead end, accumulating so many mutations and chromosomal glitches—specifically losing the X chromosome like a misplaced set of keys—that the newest pups started dying within 24 hours of birth. It turns out that while we can play God with a pipette for a while, Muller's Ratchet eventually comes for us all, proving that asexual reproduction is basically a long-form way of inviting a mutational meltdown to dinner. The takeaway? Sexual reproduction isn't just for dating apps; it’s the only thing keeping mammals from becoming a glitchy, extinct 404 error.

Less Than 3 Weeks To Go!
19 days. 300 seats. One comedy club.
ResusX 2026 starts May 18 in Philadelphia — and unlike a hotel ballroom, the Punch Line doesn't scale. When the room fills, it fills.
What you'll be in the room for:
→ Live procedural demos. Not clips.
→ Expert debates that actually move the needle.
→ Cases where you're the one making the call.
→ Heavy content. Unforgettable room.
If you've been telling yourself you'll level up your resus skills "soon" — there is no later this year. There's just this.
→ Not an attending? You're invited too. Get your discount code here

The One Thing That Should Always Follow An MTP
Here's something that gets missed more than it should during massive transfusions: calcium. When you're running a massive transfusion protocol, those packed RBCs come loaded with citrate — and citrate chelates calcium, driving your patient into hypocalcemia before you even realize it. Don't wait for a lab value to confirm it. You don't have that luxury when someone is hemorrhaging in front of you. The rule is simple: for every two to three units of PRBCs, give two to three grams of calcium gluconate. Make it automatic.
The reason this matters so much comes down to three things that you absolutely cannot afford to compromise in a critically ill, hemorrhaging patient. First, hypocalcemia causes cardiac depression — that means lower blood pressure in someone who is already hemodynamically unstable. Second, calcium is essential for coagulation, and the whole point of your massive transfusion is to help this patient clot. Third, these patients are already at elevated risk for arrhythmias, and hypocalcemia pours fuel on that fire. Calcium gluconate is cheap, it's easy to give, and it could be the difference-maker. Give. The. Calcium. Write it on your hand if you have to.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or LinkedIn accounts.


Osmotherapy is a cornerstone of neurocritical care, primarily guided by the Monro-Kellie Doctrine, which dictates that because the skull is a rigid container, any increase in brain volume must be compensated for by a decrease in CSF or blood to prevent rising intracranial pressure (ICP). The treatment works by creating an osmotic gradient that pulls water out of the brain tissue and into the vasculature. Clinicians typically utilize a tier-based approach, starting with basic critical care measures before escalating to osmotic agents like mannitol (the "sugar") or hypertonic saline (the "salt"). While mannitol is a classic choice that induces osmotic diuresis, it carries risks of hypovolemia and "rebound" ICP elevation; consequently, many modern practitioners favor hypertonic saline for its ability to maintain hemodynamics and provide a more sustained reduction in pressure.
Recent clinical perspectives are shifting traditional dogmas, particularly regarding administration and alternative agents. While 23.4% hypertonic saline was historically restricted to central line access, emerging data suggests it can be safely administered via peripheral IV in emergencies, such as a "blown pupil" scenario, with minimal risk of permanent tissue damage. Furthermore, sodium bicarbonate is gaining traction as a viable off-label osmotic agent because it lacks the chloride load that can lead to metabolic acidosis. Ultimately, the choice between agents often depends more on the patient’s specific side-effect profile—such as avoiding mannitol in hypovolemic stroke patients—than on definitive head-to-head outcome data, as large-scale trials like the Sugar or Salt (SOS) study continue to seek more conclusive evidence.
Check out this video of Dr. Brian Wright from ResusX:2025 now!

 Does Rivaroxaban Actually Cause More Bleeding?
Does Rivaroxaban Actually Cause More Bleeding?
Choosing between apixaban and rivaroxaban for acute venous thromboembolism has long been a coin flip — clinical guidelines have never favored one over the other because head-to-head data simply didn't exist. The COBRRA trial, however, finally changes that. Researchers conducted an international, prospective, randomized, open-label trial with blinded endpoint assessment, assigning 2,760 patients with acute symptomatic pulmonary embolism or proximal deep-vein thrombosis in a 1:1 ratio to receive either apixaban or rivaroxaban for 3 months. Clinically relevant bleeding — a composite of major or clinically relevant nonmajor bleeding — occurred in 3.3% of apixaban-treated patients versus 7.1% of those on rivaroxaban (RR 0.46; 95% CI, 0.33–0.65; P<0.001). Major bleeding was particularly striking, occurring in only 0.4% of apixaban patients compared to 2.4% on rivaroxaban — a sixfold difference. Crucially, recurrent symptomatic VTE rates were nearly identical between groups (1.1% vs. 1.0%), confirming the bleeding advantage came without any cost to thrombotic protection.
The mechanism behind this difference isn't fully established, but the timing offers a strong clue: most of the bleeding divergence appeared during the first three weeks of treatment — precisely the window when rivaroxaban is dosed at 15 mg twice daily, 50% higher than its maintenance dose. The trial has meaningful limitations, including an open-label design that could introduce ascertainment bias, data collection restricted to the first 3 months, and exclusion of patients with cancer-associated thrombosis or body weight over 120 kg. Still, for the broad population of patients presenting with acute DVT or PE, the evidence now clearly supports apixaban as the preferred DOAC.
My Takeaway Points:
-
Finding - Clinically relevant bleeding occurred less in the apixaban arm compared to rivaroxaban (3.3% vs. 7.1%, RR 0.46, P<0.001), with a sixfold difference in major bleeding between the two treatments (0.4% vs. 2.4%)
-
Practice Impact - Guidelines currently recommend DOACs equally for acute VTE — this trial provides the first robust RCT evidence to preferentially support apixaban, particularly during the acute treatment phase
-
Population - Adults with symptomatic acute proximal DVT or segmental/proximal PE; excludes patients with cancer-associated thrombosis, CrCl <30 mL/min, weight >120 kg, or atrial fibrillation
-
Limitation - Open-label design, predominantly Canadian/White population, only 3-month follow-up, and the trial was not powered to detect differences in recurrent VTE — results should not be extrapolated to cancer-associated thrombosis or extended anticoagulation indications
Want to learn more? Read the full trial Bleeding Risk with Apixaban vs. Rivaroxaban in Acute Venous Thromboembolism by L. Castellucci, et al. in the New England Journal of Medicine.
GLP-1 Agonist Overdose in the ED: What Actually Happens?
With the explosion in use of GLP-1 receptor agonists like semaglutide, dulaglutide, and tirzepatide for diabetes and weight loss, emergency departments are increasingly seeing patients after dosing errors or unintentional exposures. A recent poison center analysis helps clarify what clinicians should expect.
The Study
A 2025 retrospective cohort study evaluated 152 emergency department patients exposed to GLP-1 or GLP-1/GIP receptor agonists reported across three poison centers between 2005 and 2023. Most exposures were unintentional therapeutic errors (78%), often involving incorrect dosing or injection mistakes.
What Symptoms Occurred?
The vast majority of symptoms were gastrointestinal:
-
Nausea: 92%
-
Vomiting: 76%
-
Abdominal pain: 18%
Other effects were less common:
-
Hypoglycemia: ~9%
-
Headache, dizziness, diarrhea: <10% each
Importantly, most symptoms resolved within 8–24 hours with supportive care.
But These Drugs Last a Week…
Many GLP-1 agonists used today are long-acting formulations designed for weekly dosing, with half-lives around 5–7 days. Despite prolonged pharmacokinetics, the study found that clinical symptoms rarely last that long. Most patients improve within a day, even though drug levels remain elevated. This likely occurs because the primary toxicity is acute gastrointestinal intolerance (delayed gastric emptying and central satiety signaling), which improves once the initial stimulation resolves.
Hypoglycemia is Rare
GLP-1 agonists stimulate glucose-dependent insulin release, so significant hypoglycemia is generally uncommon when used alone. However, this study reported hypoglycemia in about 9% of patients, higher than previously reported poison center data.
Potential contributors include:
-
Delayed gastric emptying
-
Reduced oral intake from nausea/vomiting
-
Fasting or exertion
How Are These Patients Managed?
Management is largely supportive:
-
IV fluids: ~56%
-
Antiemetics: ~51%
-
Dextrose for hypoglycemia when needed
Most patients require observation only, with symptom improvement within the first day.
Practical ED Takeaways
-
Expect GI toxicity. Nausea and vomiting dominate these presentations.
-
Symptoms usually resolve quickly. Most patients improve within 8–24 hours, even though the drugs have long half-lives.
-
Monitor glucose. Hypoglycemia is uncommon but can occur, particularly with poor oral intake.
-
Education prevents accidental overdose. Most cases stem from administration errors or dosing mistakes.
Bottom Line
As GLP-1 agonist use continues to surge, ED presentations for dosing errors and exposures will likely increase. Fortunately, most cases involve self-limited gastrointestinal toxicity requiring supportive care and short observation, though clinicians should remain vigilant for hypoglycemia.
Review this week's Dose on IG or Tiktok.
----------
Dr. Abbi Briscoe is an emergency department clinical pharmacist, pharmacy residency program coordinator, and affiliate professor in Montana. She is passionate about Emergency Medicine and Critical Care education, and is an avid mountain biker and skier in her free time.
Connect with Dr. Briscoe: @lilpharm2026 (IG) or @lilpharm2026 (Tiktok)
Watch the April Videos Now!
If you're an All-Access member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring:
- Rezaie on "How High Can You Go?"
- Repanshek on "Crashing Anaphylaxis"
- Wright on "The Rapid Neuro Exam"
- Quazi on "Resuscitative Hysterotomy"
- Swaminathan on "Fast AF (How Do You Manage Atrial Fibrillation)"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW!


Responses