
Haney's Welcome
(Click image below)

![]()
Proof That Doctors Sometimes Just Made Stuff Up
Before Karl Landsteiner figured out blood types in 1901 and saved us all from playing biological roulette, 19th-century medicine was basically just vibes and wild guesses. Faced with patients bleeding out and no real way to bank blood without it coagulating into a gelatinous mess, some physicians decided the next logical step was… dairy. The theory was that because milk is nutrient-dense and, you know, white, the body would totally just convert that lactose and fat into "white corpuscles." Drs. James Bovell and Edwin Hodder kicked this off in 1854, and while their first few patients somehow survived (a miracle of sheer luck or small volumes, surely), it didn't take long for the rest of the medical community to realize that intravenous calcium and fat are not, in fact, a balanced breakfast for the human circulatory system.
Predictably, the "milk drip" trend went downhill fast. Patients started presenting with chest pain, rapid-fire nystagmus, and a sudden, regrettable tendency to slip into a coma and die. Even when researchers tried to pivot to human milk to avoid "animal incompatibility," the results remained spectacularly lethal—mostly leading to the immediate arrest of the patient's respiratory drive. It took until the late 1880s for the medical establishment to finally admit that injecting dairy into veins wasn't quite the panacea they hoped for. We eventually got blood banking right, but let’s be real: the fact that we once tried to cure anemia with a tall glass of cow’s milk is exactly the kind of unhinged energy that makes medical history so gloriously terrifying.
ResusX:2026 Might Be Over, But The Education Isn't.
ResusX:2026 wrapped up last month. It was an incredible experience. Three days, live in Philadelphia. A room full of diverse clinicians who take resuscitation very seriously.
Whether you watched it live and want to revisit every moment, or you couldn't make it and need to catch up — the content is here, and it's yours for life.
Every session. Every debate. Every faculty Q&A. AVAILABLE NOW!
And don't forget...new ResusNation Membership tiers are coming in July 2026! More CME, more clinical depth, and more access to the education that actually moves the needle in resuscitation medicine.
NODES: The Mnemonic That Could Save Your Next Patient
You gave the D50, mental status improved, and you're feeling good about the save — but you're not done. The most common mistake I see is clinicians stopping there and not asking the critical follow-up question: why is this patient hypoglycemic? When it's not insulin misuse or a sulfonylurea, you need a systematic approach, and that's where my NODES mnemonic comes in: Neoplastic, Organ dysfunction, Drugs/toxins, Endocrine, and Sepsis. Insulinomas, large sarcomas secreting IGF, cirrhosis tanking gluconeogenesis and glycogen stores — these are the diagnoses you will miss if you close the chart after the glucose corrects.
The one that should keep you up at night? Sepsis. Hypoglycemia in the setting of sepsis signals a dramatically worse prognosis and demands immediate, aggressive resuscitation — early antibiotics, source control, the whole package. And don't sleep on adrenal insufficiency either; when cortisol can't counter insulin, you're in trouble. Fix the sugar fast, but your very next move has to be hunting down the cause.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or LinkedIn accounts.

Dr. Sara Crager details a high-stakes trauma management scenario where a 21-year-old severe trauma patient presents to the emergency department with life-threatening hypoxemia, saturating at just 70% despite the current ventilator settings (FiO2 of 100, PEEP of 10). She contrasts the unpredictable, heterogeneous nature of trauma-induced lung injuries with standard ARDS cases, emphasizing that traditional, uniform ARDSnet protocols often fail in trauma environments. Instead, the clinician must treat the ventilator as an immediate diagnostic tool rather than a passive therapeutic device, using the paralyzing window right after intubation to accurately read waveforms and gauge underlying physiology.
Dr. Crager’s lecture provides a structured algorithmic framework for troubleshooting respiratory pressures by dissecting the distinct clinical meanings behind peak and plateau pressures. A simultaneous rise in both peak and plateau pressures signals a compliance emergency such as an untreated pneumothorax, abdominal compartment syndrome, or severe pulmonary contusions. Conversely, a spike in peak pressure with a normal plateau pressure indicates an airflow resistance issue, frequently caused by blood clots obstructing the endotracheal tube or bronchi--a state requiring urgent bronchoscopy or nebulized TXA. She also reviews practical bedside maneuvers to optimize ventilation-perfusion (VQ) matching, including placing the patient in reverse Trendelenburg, positioning the good lung down to exploit gravity-led blood flow, utilizing volume-targeted pressure control for air leaks, and meticulously titrating PEEP to avoid hemodynamic collapse or worsening an occult pneumothorax.
Check out this video of Dr. Sara Crager from ResusX:2026 now!


Why Routinely Reaching for Bicarb During IHCA is the Wrong Move
Despite physiologic rationale suggesting acidosis impairs catecholamine response and cardiac contractility, clinical evidence for sodium bicarbonate in cardiac arrest has always been weak — yet it's been given in more than half of all in-hospital cardiac arrests in the U.S. The BIHCA trial finally put this to a rigorous test: a randomized, double-blind, placebo-controlled study across 21 Danish hospitals enrolling 779 adults with in-hospital cardiac arrest, comparing up to 100 mmol of IV sodium bicarbonate against placebo, with sustained ROSC (≥20 minutes) as the primary endpoint.
The results were unambiguous. ROSC occurred in 39% of the bicarbonate group versus 37% of placebo (RR 1.05; 95% CI 0.88–1.24; P = .62), with no significant differences in 30-day survival or neurologically favorable outcome. Bicarbonate did change the biochemistry — post-arrest pH rose, alkalosis occurred in 35% versus 20%, and hypernatremia in 42% versus 29% — but without any clinical benefit. Critically, the trial achieved median drug delivery at just 8 minutes, far earlier than prior studies, eliminating the timing excuse. The confidence intervals are narrow enough to rule out a clinically meaningful effect on ROSC. For clinicians who have been giving bicarb as a reflex during prolonged codes or acidotic arrests, this trial provides the definitive RCT evidence that current guidelines have lacked. Routine sodium bicarbonate administration during in-hospital cardiac arrest should stop.
My Takeaway Points:
- Finding - Sodium bicarbonate did not improve sustained ROSC compared to placebo (39% vs 37%; RR 1.05; 95% CI 0.88–1.24; P = .62), with no significant differences in 30-day survival or neurologically favorable outcomes in the first RCT of its kind for in-hospital cardiac arrest.
- Practice Impact - Routine administration of sodium bicarbonate during in-hospital cardiac arrest should be discontinued — the drug altered post-arrest biochemistry (higher pH, higher sodium) without translating into any clinical benefit, while increasing rates of alkalosis and hypernatremia; reserve bicarb for specific indications such as hyperkalemia or tricyclic overdose.
- Population - Adults (median age 73 years) experiencing in-hospital cardiac arrest requiring epinephrine, enrolled across 21 Danish hospitals; 88% had non-shockable initial rhythms (PEA or asystole), and 64% arrested on standard medical or surgical wards — closely mirroring the real-world IHCA population.
- Limitation - The trial was powered to detect a difference in ROSC, not long-term survival or neurologic outcomes, and even the trend toward better 30-day survival (12% vs 9.1%) cannot be definitively interpreted; additionally, the exclusively Danish setting and inability to measure intra-arrest pH prior to enrollment limits generalizability to populations with variable acidosis burden or different resuscitation infrastructure.
Want to learn more? Read the full paper Sodium Bicarbonate for In-Hospital Cardiac Arrest: A Randomized Clinical Trial by A. Granfeldt, et al. in JAMA.
Aspiration ≠ Pneumonia: Why Antibiotics are Often Unnecessary
This week Dr. Jain argues that aspiration pneumonitis and aspiration pneumonia are two biologically distinct entities that clinicians routinely conflate, leading to widespread antibiotic overuse. Aspiration pneumonitis is a non-infectious chemical injury from sterile gastric contents that typically improves within 24 to 48 hours with supportive care alone — multiple studies show empiric antibiotics provide no benefit in this setting. Aspiration pneumonia, by contrast, is a true infection from inhaled oropharyngeal bacteria, has a delayed onset beyond 48 hours, and is the only entity that actually requires antibiotics. The reflex to treat every aspiration event with antibiotics — driven by early fever, infiltrates, and fear of deterioration — is described as one of the most common drivers of inappropriate antibiotic use in emergency and acute care.
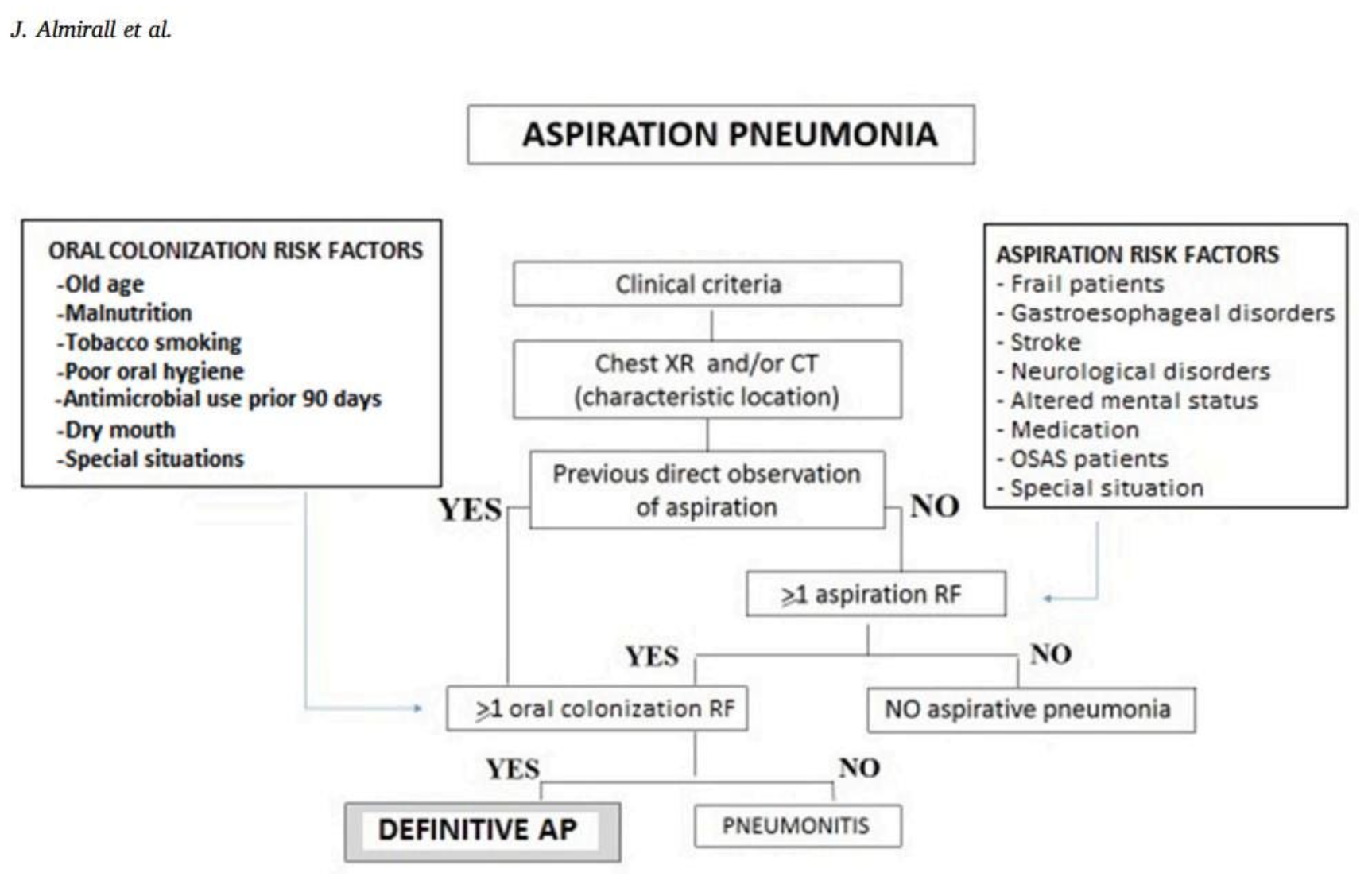
He also challenges several common clinical shortcuts. Imaging (chest X-ray, CT, and even lung ultrasound) can confirm lung involvement but cannot distinguish chemical injury from true infection, making ultrasound-triggered antibiotic prescribing a stewardship error. Guidelines from the Infectious Diseases Society of America (IDSA) and BMJ Best Practice do not recommend routine anaerobic coverage for aspiration events — clindamycin or metronidazole should be reserved only for lung abscess, empyema, or necrotizing pneumonia, not reflexively added after any aspiration. The practical takeaway: hold antibiotics if symptoms are improving and the event occurred within 48 hours, start them only if there is clinical deterioration or persistence beyond that window, and prioritize early de-escalation. Overtreatment in these cases is linked to multidrug-resistant organisms, longer hospital stays, and higher complication rates with no mortality benefit.
Read the full post here and review this week's Frontline clinical pearls on IG.
----------
Dr. Arihant Jain is an Emergency Medicine physician at All India Institute of Medical Sciences (AIIMS) in New Delhi, and the creator of Life on the Frontline, a blog sharing concise, evidence-based insights from the ED. He currently serves as a Decision Editor for CPC-EM, is among the youngest ATLS faculty in India, and an AHA-certified BLS/ALCS instructor.
Connect with Dr. Jain: @humans.of.em (IG)
Watch the June Videos Now!
If you're an All-Access member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring:
- Repanshek on "Crush Injuries"
- Hagahmed on "Peri-Arrest Pearls & Pitfalls"
- Mallemat & Swaminathan on "A Curious Case of Resuscitation"
- Haywood on "The Art of Pre-Oxygenation"
- Kim on "A Practical Approach to Massive Transfusion"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW!


Responses