
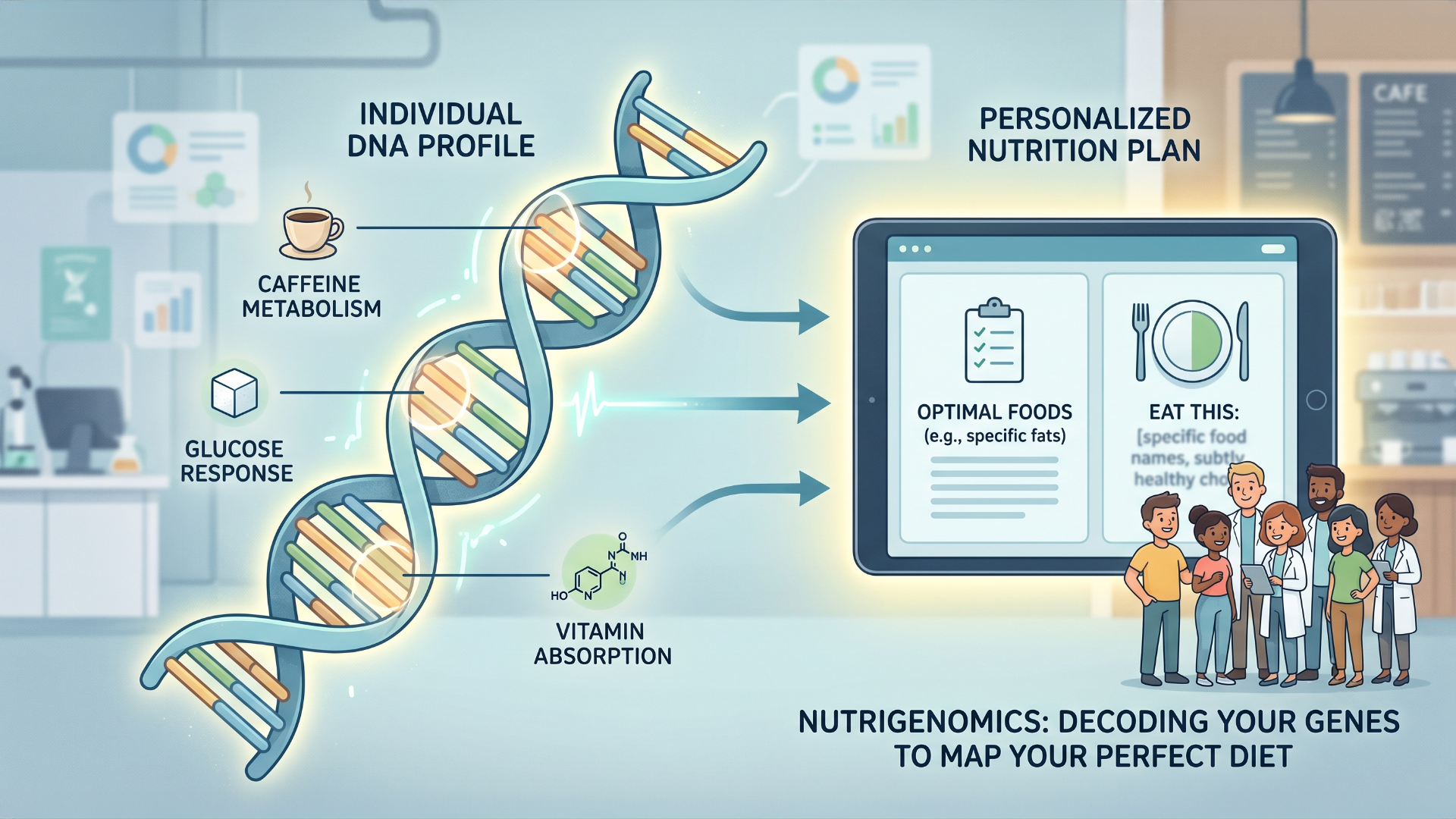
Is Your Genome Eating Better Than You Are?
So, you’ve probably seen the ads—the ones promising that if you just send a vial of spit to a lab, they’ll tell you exactly why you can’t lose those last five pounds or why you’re a jittery mess after a single espresso. That’s the "Wild West" of nutrigenomics, a field that’s currently trying to bridge the gap between hard-core molecular biology and the wellness-influencer-industrial complex. At its core, the science is actually fascinating; we’re talking about mapping how single nucleotide polymorphisms (SNPs) dictate whether you’re a "slow metabolizer" of caffeine, or if you’ve got the GLUT2 "sweet tooth" variant that makes sugar hit your brain differently. It’s the ultimate version of "it’s not you, it’s your genome," giving us a glimpse into a world where we could eventually swap the generic "eat more kale" advice for highly tailored, bio-specific dietary blueprints that actually make sense on a cellular level.
But, before you start rewriting your patient’s diet plans based on a direct-to-consumer report, remember that we’re currently in the "everything is a correlation" phase of this technology. While there’s undeniable, cool science happening in labs to understand nutrient-gene interactions, much of what’s being marketed right now is a jump from "we found an association" to "buy this supplement to fix your gene expression." The reality is that metabolism isn't just one gene; it’s a chaotic, beautiful symphony involving your microbiome, your epigenome, and the fact that most people’s "dietary interventions" are still governed by socioeconomic status rather than their specific DNA profile. It’s a field with massive promise, but for now, the gold standard remains the boring stuff: quality sleep, movement, and eating actual food, not just the stuff your saliva test told you to buy.
Last Week For
Early-Bird Registration
A new conference is coming this fall, and I think you're going to love it.
EMX is a brand-new emergency medicine conference I'm co-hosting with Dr. Anand Swaminathan — built for clinicians who want the whole emergency department sharpened, not just one narrow slice. Cardiology, stroke, peds, tox, endocrine, OB, MSK, airway — whatever walks through your door, EMX gets you ready for all of it.
For our inaugural meeting, EMX will be held virtually — so no matter where you practice, you can be there. Everything else you'd expect from a world-class conference? Still here.
And this isn't your standard lecture marathon. We're talking talk-show interviews, live media reads, real expert debates, audience polling — and our signature 🔥 Hot Ones segment. You'll be locked in from the first slot to the last.
The faculty lineup includes Amal Mattu, Reuben Strayer, Evie Marcolini, Tarlan Hedayati, Jenny Beck-Esmay, and more of the clinicians who actually shape how emergency medicine is practiced.
📅 September 15–16, 2026 | Virtual / Online
📍 ✅ 9.5 CME/CEU Credits
Want to add a full afternoon with Amal Mattu + 3.5 CME/CEU credits? Grab a virtual seat at the ECG Pre-Conference Workshop on September 14 — limited to 50 people.
🎟️ Early-bird pricing is live right now — and it won't last long.

We're launching new membership tiers built for clinicians who want more — more CME, more clinical depth, and more access to the education that actually moves the needle in resuscitation medicine.
Before we open the doors, we're giving you one more chance to experience it FREE. Join us on July 20, 2026 @ 4PM EST for a complimentary, virtual Grand Rounds session and get a front-row seat to exactly what ResusNation membership looks like in practice. No cost, no commitment — just high-yield clinical education, the way it should be.
This is your last chance to join a Grand Rounds for free before the new memberships launch. July Grand Rounds will feature Mohamed Hagahmed, MD as he delivers a focused, clinically actionable breakdown challenging the way we think about traumatic cardiac arrest — one talk you don't want to miss!

3 Key Tips for Calling Consults
I work in the ER and the ICU, and calling consults is a huge part of my day — so let me give you three tips that will immediately level up how you do it. First: never apologize for calling a consult. That person is literally paid to be in the hospital and do consults. When you open with an apology, you've already positioned yourself from weakness. Instead, be polite and direct: "Hi, is this surgery? Do you have a moment for a consult I have in the ICU?" Second: lead with the question. I constantly overhear people rattling off a 49-year-old with diabetes, hypertension, heart failure, peripheral edema — and none of it has anything to do with the actual issue. Start with "I have a 49-year-old male with right lower quadrant pain and I'm concerned about appendicitis," then add your history flavor after.
Third: ask when they anticipate seeing the patient. They're busy, you're busy — but closing that loop is fair game. Sometimes they won't know, and that's fine. But setting the expectation usually gets them to at least tell you if they're delayed, so you can update your team and your patient.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or LinkedIn accounts.

Reuben Strayer, MD delivers a compelling, contrarian critique of the Advanced Trauma Life Support (ATLS) protocol, arguing that while rigid, sequential algorithms are invaluable for solo, novice, or non-trauma clinicians, they actively degrade the performance of experienced trauma specialists. By forcing experts to treat every case under a "worst-case scenario" assumption, traditional ATLS guidelines often lead to rigid, over-protocolized care that can cause unintended harm. The talk highlights a critical paradigm shift in medicine: algorithms establish a safe baseline for beginners but create an artificial ceiling for experts who should instead rely on nuanced, adaptive, and synchronized team-based clinical reasoning.
To illustrate this, Dr. Strayer breaks down major updates in the 11th edition of ATLS that finally align with what modern emergency medicine practitioners have known for years. Key systematic failures of past editions are thoroughly dismantled—such as the dangers of early intubation in hypoperfused patients, the hidden harms of unnecessary cervical spine immobilization, and the historical misuse of large crystalloid fluid volume resuscitation (now updated to zero liters for exsanguinating patients). By calling out obsolete defensive practices like routine log rolls and digital rectal exams, he advocates for a thoughtful, personalized approach to trauma care, positioning the expert emergency physician not just as a protocol-follower, but as a critical advocate protecting the patient from systemic over-intervention.
Check out this video of Dr. Reuben Strayer from ResusX:2026 now!


Does 2g of Mag Speed Lactate Clearance in Sepsis?
Lactate clearance during septic resuscitation is usually framed as a fluids-and-pressors problem, but a triple-blind RCT from AIIMS Jodhpur tested whether adding IV magnesium sulphate could speed it up. Among 138 Sepsis-3 adults with lactate above 2 mmol/L, 2 g of magnesium daily for three days cut time to 20% lactate clearance nearly in half (5.73 vs 8.54 hours, P < 0.001), with the gap widening each day through day 3 (50.74% vs 37.94% clearance).
The benefit tracked downstream too: lower vasopressor doses on days 2–3, ICU stay down from 12 to 8 days, hospital stay down from 16 to 12 days, and no adverse events — though 28-day mortality (21.7% vs 34.8%, P = 0.12) wasn't statistically significant.. So what changes tomorrow? Not much, yet. This is a modest, single-site trial with a metabolic surrogate as its endpoint, and it doesn't establish that faster lactate clearance saves lives. But magnesium is cheap, familiar, and was well tolerated here, and the signal across clearance, pressor dose, and length of stay is consistent enough to justify a properly powered multicentre trial. Worth noting for anyone already reaching for magnesium in the septic patient with borderline levels — this study offers the first randomized support for that instinct, not permission to make it routine.
My Takeaway Points:
- Finding - Time to 20% lactate clearance was 5.73 hours with magnesium vs 8.54 hours with placebo (mean difference −2.81 h, 95% CI −3.65 to −1.99, P < 0.001), with day-3 clearance of 50.7% vs 37.9%.
- Practice Impact - Adjunctive 2 g IV magnesium sulphate daily × 3 days was associated with lower vasopressor doses on days 2–3, ICU stay shortened from 12 to 8 days, and hospital stay from 16 to 12 days — with no adverse events observed.
- Population - 138 adults (n = 69 per arm) with Sepsis-3 sepsis and lactate > 2 mmol/L in a single tertiary ICU in India; patients with chronic renal impairment, liver failure (Child-Pugh B/C), DKA, metformin use, alcoholism, pregnancy, or refractory hypotension (MAP < 65 on pressors) were excluded.
- Limitation - Baseline serum magnesium was never measured, so it's unclear whether the benefit reflects correcting deficiency or a pharmacologic effect. Single-centre design, no renal replacement therapy data, and 28-day mortality (21.7% vs 34.8%) that was underpowered and nonsignificant.
Want to learn more? Read the full study Impact of Magnesium on the Clearance of Lactate in Critically Sick Patients with Sepsis: Randomized Clinical Trial by C. Anbarasan, et al. in World Journal of Critical Care Medicine.
The Patient Who Showed ‘Signs of Life’ During CPR
This week Dr. Jain tackles CPR-induced consciousness (CPRIC) — signs of awareness during ongoing chest compressions despite no spontaneous circulation: eye opening, purposeful movement, speech, grimacing, resistance to rescuers — all of which vanish the moment compressions stop. Observational data put the incidence around 0.23–0.9% of resuscitations, though surveys suggest roughly half of prehospital clinicians have witnessed it at least once. The physiology is straightforward once you accept that arrest is a process rather than a switch: compressions good enough to perfuse the cortex can transiently sustain higher neurological function. Parnia's AWARE-II study reinforced this, showing organized EEG activity — delta, theta, alpha — persisting 35 to 60 minutes into resuscitation. Counterintuitively, CPRIC tracks with better outcomes: higher ROSC, better survival to discharge, witnessed arrests, shockable rhythms, early CPR. It may be a physiological success signal, not a failure.
The uncomfortable half is what it costs everyone involved. Around 39% of interviewed AWARE-II survivors described experiences suggestive of consciousness during CPR, and Jaffe et al. found higher rates of depression and possible PTSD among those who recalled awareness. Providers report hesitation to continue compressions, emotional distress, intrusive recollections, and insomnia. Sedation is the obvious answer and also a trap — ketamine, fentanyl, midazolam, and restraint are all in use, but sedatives worsen hypotension in a state already dependent on compressions, and no universally accepted international guidelines exist. Dr. Jain's practical stance: recognize CPRIC early and confirm with POCUS rather than stopping compressions repeatedly, protect uninterrupted high-quality CPR as the priority, sedate only when agitation genuinely compromises resuscitation or defibrillation, build in team debriefing, and resist premature termination — because CPRIC is itself indirect evidence that compressions are perfusing the brain. The question is no longer whether consciousness can occur during CPR, but what responsibility we carry now that we know it can.
Read the full post here and review this week's Frontline clinical pearls on IG.
----------
Dr. Arihant Jain is an Emergency Medicine physician at All India Institute of Medical Sciences (AIIMS) in New Delhi, and the creator of Life on the Frontline, a blog sharing concise, evidence-based insights from the ED. He currently serves as a Decision Editor for CPC-EM, is among the youngest ATLS faculty in India, and an AHA-certified BLS/ALCS instructor.
Connect with Dr. Jain: @humans.of.em (IG)
Watch the July Videos Now!
If you're an All-Access member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring:
- Hedayati on "Right Bundle - When to be Afraid"
- Murali on "How to Depressure-Eyes"
- Hockstein on "Anti-Dysrhythmics in the ICU"
- Trott on "Adrenal Insufficiency"
- Reilly on "T-Waves You Can't Miss"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW!


Responses