
Haney's Welcome
(Click image below)
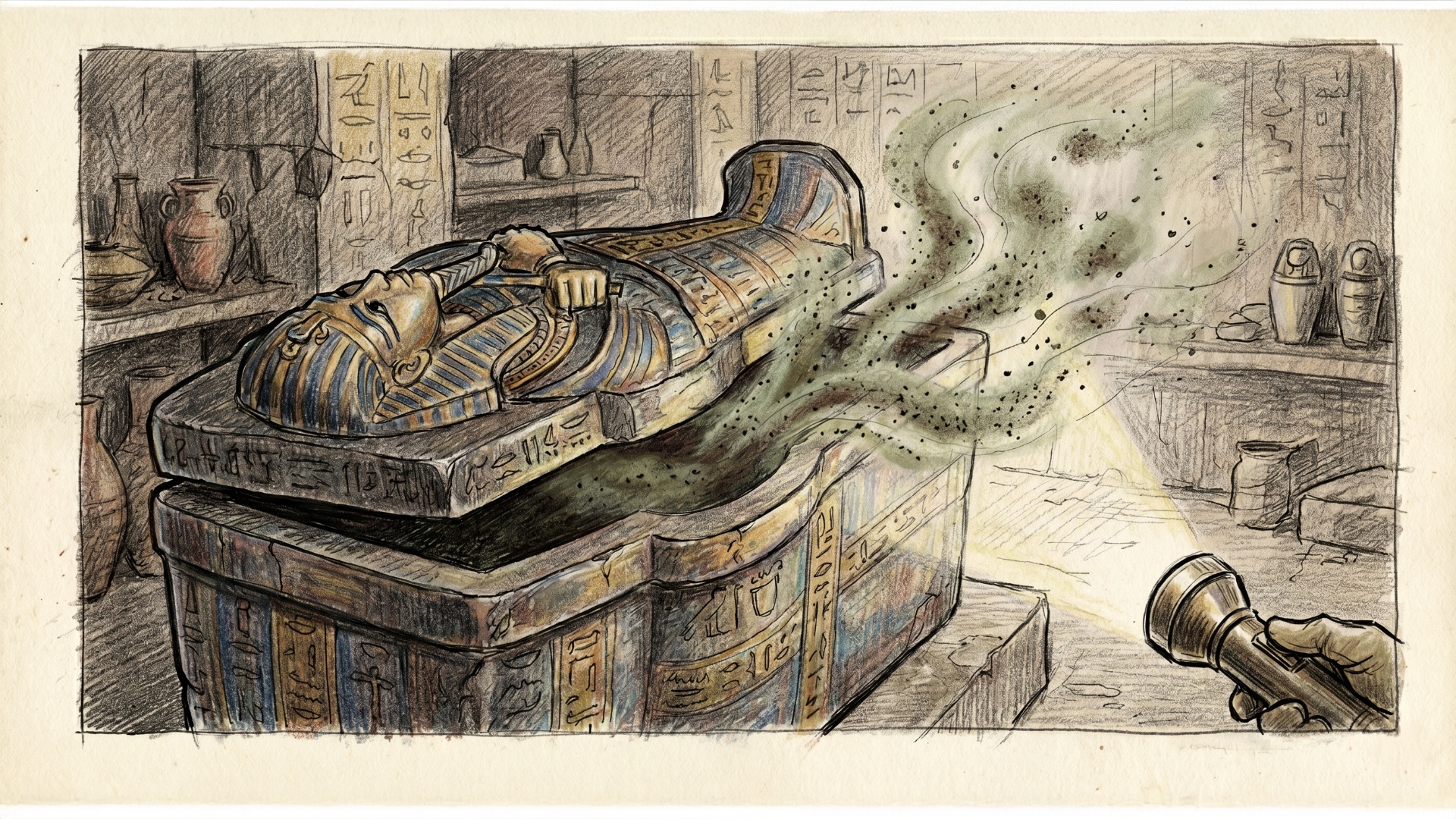
Is It Ancient Magic Or Just Opportunistic Infection?
Picture this: It's 1922, and English archaeologist Howard Carter just cracked open King Tut’s tomb, unleashing what the tabloids dramatically dubbed the "mummy’s curse" after a bunch of high-profile visitors mysteriously dropped dead. For a century, people thought ancient pharaohs were out here dealing post-mortem psychic damage, but it turns out the real culprit was just Aspergillus flavus thriving in the ultimate poorly ventilated workspace. When Lord Carnarvon swaggered into that sealed burial chamber, he wasn't hit by a dark magical hex; he inhaled a massive cloud of toxic mold spores that had been aggressively marinating in ancient grain dust for three millennia. Given that his immune system was already basically held together by duct tape after a nasty car crash years prior, he was the perfect host for an invasive fungal sinusitis that eventually spiraled into fatal pneumonia. Honestly, it’s the most classic Infectious Disease consult ever: "Patient presents with shortness of breath and an ancient Egyptian hex. Requesting pharmacy approval for voriconazole."
And if you think this was just a one-off King Tut problem, fast forward to 1973 when twelve conservationists popped open the tomb of a 15th-century Polish king. Ten of them died shortly after, which sounds like the plot of an A24 horror movie but was actually just A. flavus going on an absolute tear. These fungal spores are extreme biological introverts—they can lay dormant in a dark, sealed crypt for hundreds of years, completely unbothered, just waiting for some breathless historian to disrupt their peace. The moment outside air hits the tomb, the spores go airborne, wrecking anyone with a weakened immune system while healthy bystanders just catch a mild cough and a cool story. So, the next time you’re explaining the complications of aspergillosis, just casually remind folks that before modern antifungals, Aspergillus was successfully masquerading as the vengeful wrath of the undead.
A new is coming this fall, and I think you're going to love it.
EMX is a brand-new emergency medicine conference I'm co-hosting with Dr. Anand Swaminathan — built for clinicians who want the whole emergency department sharpened, not just one narrow slice. Cardiology, stroke, peds, tox, endocrine, OB, MSK, airway — whatever walks through your door, EMX gets you ready for all of it.
For our inaugural meeting, EMX will be held virtually — so no matter where you practice, you can be there. Everything else you'd expect from a world-class conference? Still here.
And this isn't your standard lecture marathon. We're talking talk-show interviews, live media reads, real expert debates, audience polling — and our signature 🔥 Hot Ones segment. You'll be locked in from the first slot to the last.
The faculty lineup includes Amal Mattu, Reuben Strayer, Evie Marcolini, Tarlan Hedayati, Jenny Beck-Esmay, and more of the clinicians who actually shape how emergency medicine is practiced.
📅 September 15–16, 2026 | Virtual / Online
📍 ✅ 9.5 CME/CEU Credits
Want to add a full afternoon with Amal Mattu + 3.5 CME/CEU credits? Grab a virtual seat at the ECG Pre-Conference Workshop on September 14 — limited to 50 people.
🎟️ Early-bird pricing is live right now — and it won't last long.

We're launching new membership tiers built for clinicians who want more — more CME, more clinical depth, and more access to the education that actually moves the needle in resuscitation medicine.
Before we open the doors, we're giving you one more chance to experience it FREE. Join us on July 20, 2026 @ 4PM EST for a complimentary, virtual Grand Rounds session and get a front-row seat to exactly what ResusNation membership looks like in practice. No cost, no commitment — just high-yield clinical education, the way it should be.
This is your last chance to join a Grand Rounds for free before the new memberships launch. July Grand Rounds will feature Mohamed Hagahmed, MD as he delivers a focused, clinically actionable breakdown challenging the way we think about traumatic cardiac arrest — one talk you don't want to miss!

The Second Vasopressor Is a Warning Sign
When I reach for a second vasopressor, that's not just a clinical escalation — it's a hard stop and a forced reset. Yes, it's time to think about a central line, and yes, it's time to have a goals-of-care conversation. But more importantly, it's the moment I use to interrogate my own thinking. Have I anchored too hard on this diagnosis? Does this patient actually have a cardiogenic component to their septic shock? Do they have a sepsis-induced cardiomyopathy that I've been completely ignoring? Or — and this is the one that keeps me honest — did they have cardiogenic shock from the start and I just called it sepsis?
The second vasopressor is a clinical alarm, but not the kind that tells you to do more of the same. It's the kind that tells you to stop and start over. Go back to basics. Ask the hard questions. Is there occult hypovolemia? Adrenal insufficiency? A thyroid storm hiding in plain sight? The diagnosis you committed to at hour one may be killing your patient at hour six. Never anchor. Always reassess.
Watch the full video here and leave a comment.
Don't forget to like and follow my IG, TikTok, YT, Facebook or LinkedIn accounts.


Melody Bishop, RRT provides a simplified, bedside-focused algorithmic approach to managing acute respiratory distress syndrome (ARDS) on the mechanical ventilator, sweeping aside a quagmire of conflicting research. She reinforces that the ventilator does not cure ARDS; it merely buys time for tissue healing while protecting fragile alveoli from secondary injury. The framework relies on 3 simple rules rooted in the 2000 ARMA trial, asserting that baseline protective parameters must apply to every intubated patient. These essential targets include protective tidal volumes of 6-8 mL/kg, maintaining a driving pressure under 15 cm H₂O, guarding against auto-PEEP, and ensuring baseline gas exchange goals are met safely before employing advanced or aggressive interventions.
The core differentiator in Bishop’s workflow is the oxygenation index, specifically highlighting a oxygenation ratio (PF ratio) of 150 as the ultimate clinical pivot point. When a patient maintains a PF ratio above 150, standard lung-protective ventilation parameters are sufficient, and advanced techniques like proning, paralysis, or extreme PEEP titration are unnecessary. However, if the PF ratio drops below 150, signaling severe ventilation-perfusion mismatch, clinicians must skip non-invasive trials, intubate early, lower oxygenation and pH expectations, and immediately implement advanced maneuvers. As a practical tool for high-acuity scenarios, the speaker details the EXPRESS trial method for optimizing PEEP, which advises clinicians to systematically add PEEP until reaching a maximum safe plateau pressure of 30 cm H₂O, ensuring maximal alveolar recruitment without inducing barotrauma.
Check out this video of Melody Bishop, RRT from ResusX:2026 now!


Is That "Opioid Withdrawal" Actually Something Far More Dangerous?
The US illicit drug supply has a new and dangerous adulterant. Medetomidine — a veterinary alpha-2 agonist first identified in the illicit fentanyl supply in Maryland in 2022 — has been driving overdose and withdrawal crises in emergency departments across Philadelphia, Pittsburgh, and Chicago. This narrative review synthesizes the pharmacology, toxicology, and early clinical experience to characterize what medetomidine intoxication and withdrawal look like and how to treat them. The syndrome is unlike anything in the standard opioid or sedative-hypnotic playbook: withdrawal can begin within 4–6 hours of last use, producing extreme vital sign derangements (HR >170, SBP >240, DBP >120), lactic acidosis, QTc prolongation, troponin elevation, and acute cardiomyopathy — with 77–90% of diagnosed patients requiring ICU admission. Critically, the medications clinicians reach for first — benzodiazepines, opioids, ondansetron — provide minimal relief, because this is an alpha-2 agonist withdrawal syndrome that bypasses GABA-ergic and opioid pathways entirely.
University of Pittsburgh Medical Center (UPMC) group's proposed treatment framework centers on 3 simultaneous interventions: 1) dopamine antagonist antiemetics (prochlorperazine, droperidol, or olanzapine — not ondansetron), 2) rapid oral loading with clonidine and standing guanfacine, and 3) early transdermal clonidine for tapering. Patients who progress require IV dexmedetomidine, often titrated above conventional ICU dosing to 2.4 mcg/kg/hr with RASS or Riker monitoring. A critical pitfall: early buprenorphine based on Clinical Opiate Withdrawal Scale (COWS) score can precipitate opioid withdrawal, because medetomidine withdrawal mimics moderate-to-severe opioid withdrawal but begins far sooner. No FDA-approved immunoassay exists — diagnosis is clinical, and recognition is the first intervention.
My Takeaway Points:
- Finding - Medetomidine withdrawal produces life-threatening sympathetic hyperactivation — with heart rates over 170 bpm and systolic pressures exceeding 240 mmHg — beginning as early as 4-6 hours after last use, and drives ICU admission in 77–90% of diagnosed patients.
- Practice Impact - Standard opioid and benzodiazepine-based withdrawal management is largely ineffective; treatment requires early, aggressive alpha-2 agonist replacement with oral clonidine loading, guanfacine, and transdermal clonidine — escalating to IV dexmedetomidine infusion for refractory cases, with dopamine antagonists (not ondansetron) for antiemesis.
- Population - People who use illicit fentanyl products in regions where medetomidine adulteration has been confirmed — including Pennsylvania, Illinois, and Maryland — particularly those with prior hospitalization for severe withdrawal, which is the strongest predictor of recurrence.
- Limitation - Evidence supporting this management protocol is derived entirely from early case series and clinical observation, not controlled trials; no validated medetomidine-specific withdrawal scale exists, point-of-care testing is unavailable in most settings, and the geographic spread of this adulterant is still evolving — making it difficult to define definitive observation periods or predict who will deteriorate.
Want to learn more? Read the full review Emergence of Medetomidine in the Illicit Drug Supply: Implications for Emergency Care and Withdrawal Management by M. Lynch, et al. in Annals of Emergency Medicine.
Build Better BiPAP
One of the most common things I see when I walk into an ICU or emergency department is a patient on BiPAP with settings of IPAP 12 cm H₂O and EPAP 5 cm H₂O.
Why 12/5? Is it "just what we do?"
The problem is that BiPAP is not a medication with a standard dose. It is a physiologic tool, and you should be titrating the pressures to the patient's physiology.
Let's break down what each setting means.
First: Think of BiPAP as Two Separate Interventions in One
1) EPAP (PEEP)
Think of EPAP as your lung recruitment pressure, also known as PEEP.
Its job is to:
-
-
Keep alveoli open
-
Increase end expiratory lung volume
-
Improve oxygenation
-
Reduce cyclic alveolar collapse
-
It establishes the baseline pressure from which every breath begins.
Patients with pulmonary edema, obesity, atelectasis, or hypoxemic respiratory failure often need more EPAP than patients with isolated hypercapnia.
2) IPAP
IPAP is your pressure support or pressure applied above PEEP during inspiration.
Pressure Support = IPAP − EPAP
This pressure difference generates inspiratory flow.
More flow generally produces:
-
-
Larger tidal volumes
-
Less respiratory muscle work
-
Lower work of breathing
-
Improved ventilation
-
Lower PaCO₂
-
Increasing IPAP is primarily a ventilation intervention, not an oxygenation intervention.
A Practical Starting Point
There is not one "correct" BiPAP setting, but a reasonable starting point for many adults is:
1) IPAP: 8 to 10 cm H₂O
-
Adjust upward while watching:
-
Respiratory rate
-
Accessory muscle use
-
Tidal volume
-
Patient comfort
Once IPAP gets into the mid to high teens, keep an eye out for gastric insufflation and aerophagia, particularly in patients without an artificial airway.
2) EPAP: 5 to 8 cm H₂O
Then individualize it.
Higher EPAP may be appropriate when the primary problem is oxygenation, alveolar collapse, pulmonary edema, or obesity.
Remember: If you raise EPAP without also raising IPAP, your pressure support shrinks.
Example:
10/5 = Pressure support of 5
10/8 = Pressure support of 2
The patient now receives substantially less inspiratory assistance despite having the same IPAP. Many clinicians unintentionally decrease ventilation while trying to improve oxygenation.
Inspiratory Time
The ventilator can only deliver volume while inspiration is occurring. A longer inspiratory time allows more time for flow, which generally increases delivered tidal volume. A shorter inspiratory time delivers less volume. Keep in mind that inspiratory time only affects machine-timed breaths. If the patient is triggering and cycling their own breaths, changing the machine's inspiratory time often has little or no effect because the patient determines breath duration through the machine's algorithm. This is something to discuss with your hospital's respiratory therapy department, as implementation varies among ventilator manufacturers.
Rise Time
Rise time determines how quickly the ventilator reaches IPAP.
A faster rise time:
-
Delivers support rapidly
-
Unloads the respiratory muscles earlier
-
May feel more comfortable for patients with high inspiratory demand
A slower rise time:
-
Provides smoother pressure delivery
-
May improve comfort in patients who dislike an abrupt pressure increase
There is no universally "correct" rise time. Match it to the patient's respiratory mechanics and comfort. But it is something you can change at the bedside as you watch the patient.
Spontaneous/Timed (S/T) Mode:
Some BiPAP devices are used in Spontaneous/Timed (S/T) mode.
In S/T mode, the patient triggers breaths whenever possible. If the patient fails to breathe, the ventilator delivers backup breaths at the programmed respiratory rate. Depending on the machine you are using, be aware that Pressure Support mode often does not have a mandatory control rate. Instead, it only provides a backup apnea rate. In CPAP mode, ventilation is entirely spontaneous, meaning the patient must have an intrinsic respiratory drive. Be cautious about placing patients who are at risk for apnea on CPAP alone. Knowing the machine you are using is just as important as knowing the physiology.
What I Watch
When I adjust BiPAP, I am much less interested in chasing a blood gas than I am in watching the patient.
-
The first signs that you are winning are often:
-
Decreased work of breathing
-
Lower respiratory rate
-
Increasing tidal volume
-
Improved mental status
-
Better patient comfort
Bottom Line
It is about understanding physiology.
Review this week's pearls on IG.
----------
Dr. Ghionni is also the creator of @pulmtoilet on Instagram and hosts The Peak Inspiration Podcast — a free resource available on YouTube, Spotify, and Apple Podcasts.
Connect with Dr. Ghionni: @pulmtoilet IG / YT / Spotify / Apple
Watch the July Videos Now!
If you're an All-Access member, you're in for some great content this month. We have FIVE videos hand-picked by our staff that are high-yield and our most highly watched. We're featuring:
- Hedayati on "Right Bundle - When to be Afraid"
- Murali on "How to Depressure-Eyes"
- Hockstein on "Anti-Dysrhythmics in the ICU"
- Trott on "Adrenal Insufficiency"
- Reilly on "T-Waves You Can't Miss"
Each month we bring you fresh new content from the best of the best in resuscitation. If you're an All-Access member, go watch these videos NOW!


Responses